
September 30, 2018
https://doi.org/10.23999/j.dtomp.2018.3.4
J Diagn Treat Oral Maxillofac Pathol 2018;2:118−21.
Under a Creative Commons license
HOW TO CITE THIS ARTICLE
Zhehulovych ZY, Fesenko II, Al-Makhamid NS. Linkows` blade-vent implants continue to work after twenty-nine years: case report. J Diagn Treat Oral Maxillofac Pathol 2018;2(3):118−21.
INSTITUTIONAL REPOSITORY
https://ir.kmu.edu.ua/handle/123456789/775
ABSTRACT
We report a case of two osseointegrated Linkows` blade-vent implants supported fixed partial dentures that still osseointegrated at the mandible of 54-yeor-old patient during last twenty-nine years. The purpose of the report is to compare the bone condition around the blade-vent implants, condition of the fixed dentures, and two abutment teeth. Benefits and disadvantages of Linkows` blade-vent implants are also highlighted.
INTRODUCTION
Endosseous blade-vent implants (related names: blade implants, Linkow-type blade implants, Linkow-type blade vent implants) were introduced by American dentist and pioneer in the field of oral implantology Leonard Linkow in 1968 [1, 2]. First 2 year follow-up results were presented by him in 1970 [3]. The whole next five decades is a period that shows a transition from wide blade-vent and subperiosteal implants usage to root-form and zygomatic implants usage not only into jaws but also into flap-reconstructed mandible/maxilla [4, 5]. A lot of publications show that, despite of disadvantages, blade-vent implants continue to work in the long time follow-up period [6-20]. One of them is Pasqualini and Pasqualini (2003) publication, who reported a success rate of 91% at 10 years for 386 blade implants placed between 1971 and 2009 [2, 7]. Risks and benefits of connecting an implant and natural tooth were precisely described by Brägger et al (2001), Cordaro et al (2005), Nickenig et al (2006), and Davis et al (2014) [21- 24]. Our case represents a unique comparison of long-term usage of two tooth-blade-vent-implant supported fixed partial dentures with different conditions of denture- supported teeth (endodontically treated vs non-treated).
CASE REPORT
A healthy 54-year-old lady referred to the Center of Maxillofacial Surgery for a one month history of movement of one of the fixed partial dentures. Out-office oral examination revealed a non-significant mobility of an anterior part of tooth-implant fixed partial denture in area of tooth 3.4 (Figs 1 and 2B) and signs of gingival inflammation in the area of contact of the movable part of the denture near root of the tooth 3.4. Mobility of the denture was caused by the destruction of crown of the abutment teeth 3.4 by caries. The tooth-implant fixed partial denture on the opposite site shows no mobility and symptoms of gingival inflammation.
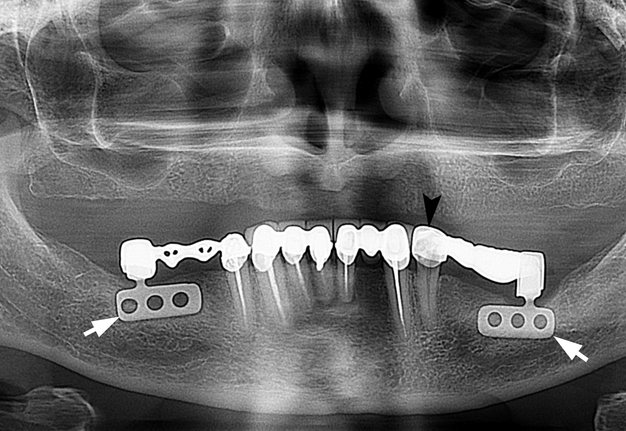
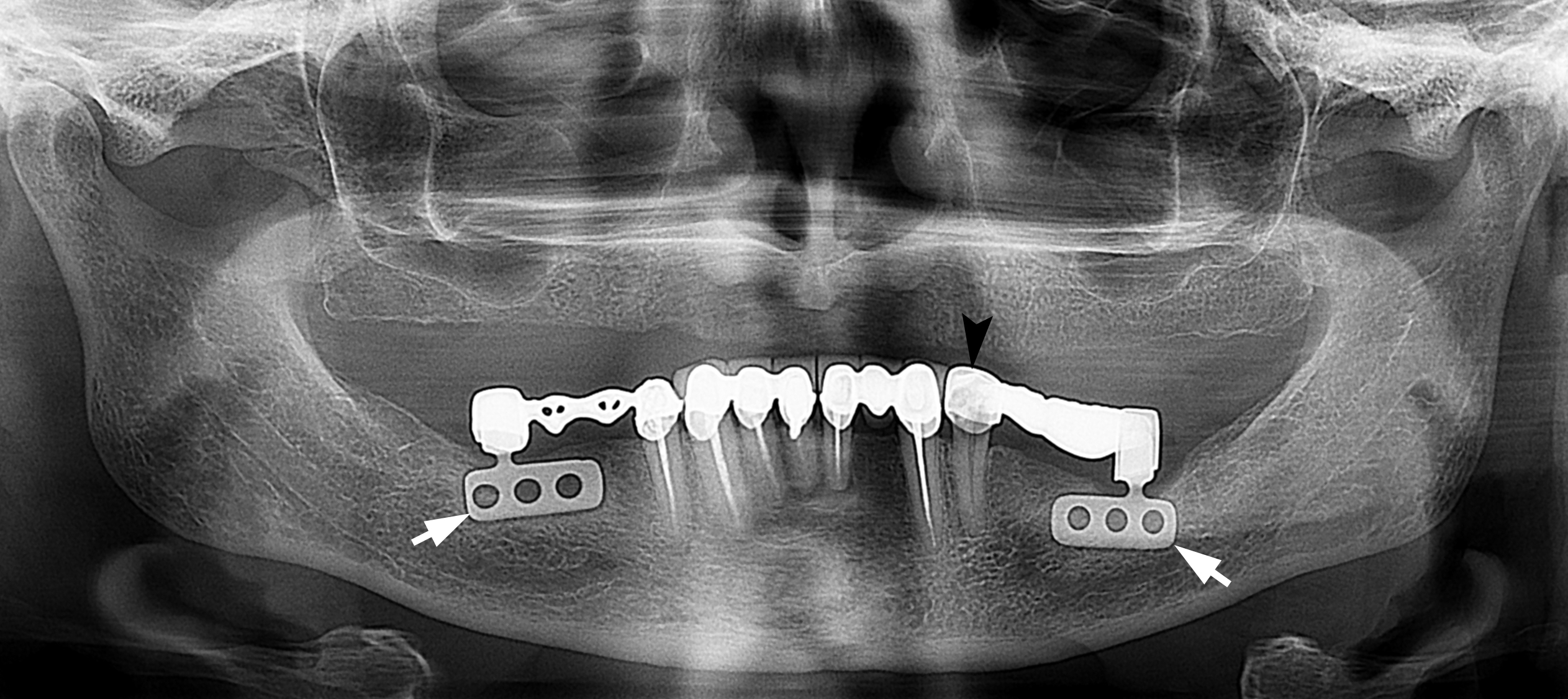
FIGURE 1. A panoramic radiograph of 54-year-old lady after 29 years of the blade-vent implants (arrows) placement. Notes the mobility (arrowhead indicates direction of mobility) of fixed bridge (cement fixation) on the tooth 3.4. Oral examination revealed a destruction of the crown part of tooth 3.4 with caries to the level of tooth neck. Radiograph shows no radiopaque filling material inside a root canal of tooth 3.4. No crestal bone resorption or peri-implant radiolucencies are present.
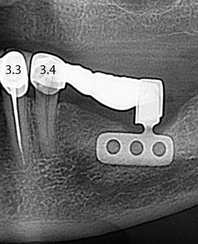
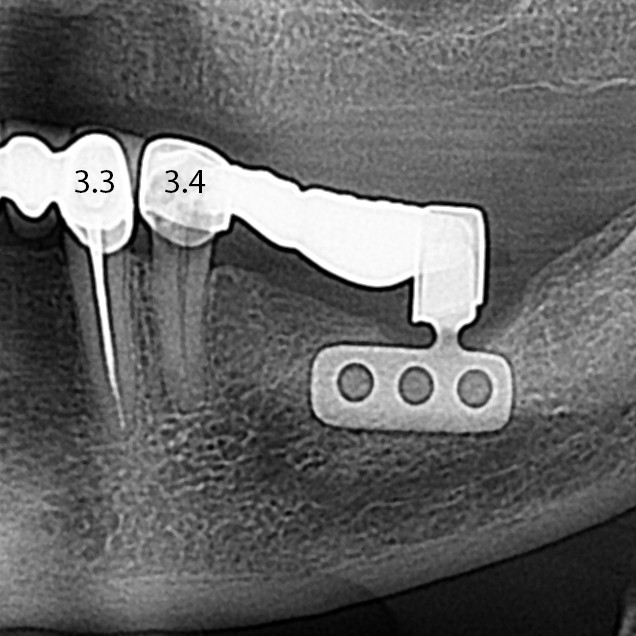
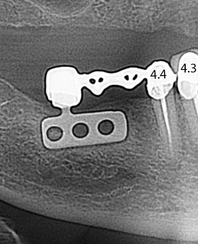
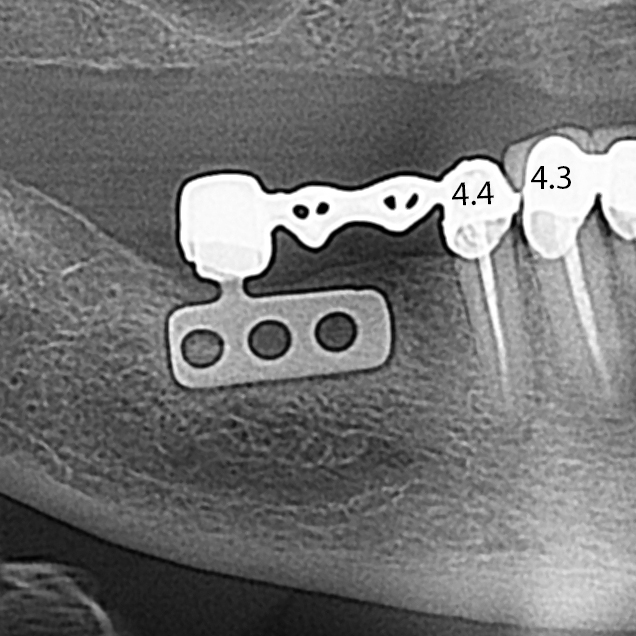
FIGURE 2. A cropped and zoomed panoramic radiograph of the same patient. The teeth are indicated by numbers. (A) Tooth-implant fixed partial denture on the right side. Denture is fixed at endodontically treated tooth 4.4. (B) Tooth-implant fixed partial denture on the left side. Denture is fixed at non-treated tooth 3.4.
A panoramic radiography (Figs 1, 2) shows two blade- vent implants with the tooth-implant supported fixed partial dentures. A good bone level at the alveolar ridge in areas of inserted blade-vent implants was noted. According to patient medical history the two blade-vent implants (there was no precise data about manufacturer; implants material is presumably titanium, taking into account the production capacity in the late 1980s and the longevity of these two implants) placement and prosthetic work were performed in 1986 at Department of Prosthetic Dentistry, Bogomolets National Medical University (Kyiv, Ukraine). Endodontic treatment of the tooth 4.4 was performed simultaneously with blade implants placement. At maxilla a patient used a fully removable denture during the whole period of dental implants function at the mandible.
The condition upon oral examination and panoramic radiography clearly demonstrate us the need of tooth 3.4 treatment with possibility to use it as abutment tooth further in new tooth-implant supported fixed partial denture.
DISCUSSION
Naert et al (2001) [25] in their study of 339 implants fixed to 313 abutment teeth, shows that complications with the implant-tooth group included: periapical lesions (3.5%), tooth fracture (0.6%), extraction (decay or periodontal disease) (1%), intrusion (3.4%), and cement failure (8%). Davis et al (2014) [24] argued about the next advantages of a tooth-implant supported fixed partial dentures: 1) increased tactile perception; 2) greater chewing comfort and efficiency; 3) avoidance of vital structures; 4) reduced cost; 5) reduced need for advanced graft; 6) improved patient acceptance.
Thus, upon the planning of the tooth-implant supported fixed partial dentures the next risks [24] cannot be ignored: 1) intrusion of natural tooth; 2) biomechanical complications: fixture-abutment failure, loss of retention, screw loosening/implant fracture (implant, especially risk is high in the neck of blade implants [26], cement failure (implant/tooth), fracture (tooth), caries (tooth), crown fracture; 3) loss of natural tooth: endodontic involvement, fracture, caries, periodontal disease; 4) peri-implantitis.
CONCLUSION
The twenty-nine years of two blade-vent implants function in implant-tooth fixed dentures confirms: 1) a possibility of blade implants to perform function; 2) to be a long-term period successfully osseointegrated; 3) to have insignificant bone resorption around the implants, showing no alveolar ridge atrophy; 4) a tooth-blade-vent- implant supported fixed partial denture can long-term exist in case of healthy/perfect endodontically treated abutment teeth.
And we are completely supporting an opinion of Davis et al (2014) [24] that for the sake of increasing predictability, cases for combination tooth-implant supported FPDs should include ideal proposed implant location, healthy natural/endodontically treated abutment teeth, and excellent patient factors such as occlusion, oral hygiene, and motivation.
Conflict of Interest
The authors declare no conflict of interest.
Role of the Authors and Co-authors
Zinaida Y. Zhehulovych (editing)
Ievgen I. Fesenko (material collection, concept of a paper, and editing)
Nadim S. Al-Makhamid (material collection and writing)
Ethical Approval
No needed.
Fundings
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors.
Acknowledgments
The authors are grateful to Sergii I. Khrulenko (x-ray laboratory assistant; Kyiv Regional Clinical Hospital, Kyiv, Ukraine) for high quality panoramic radiography (images of Figs 1, 2).
REFERENCES (26)
-
Linkow LI. The blade vent – a new dimension in endosseous implantology. Dent Concepts 1968;11(2):3–12.
-
Pasqualini U, Pasqualini ME. Treatise of implant dentistry: the Italian tribute to modern implantology. Carimate: Ariesdue; 2009.
-
Linkow LI. Endosseous blade-vent implants: a two-year report. J Prosthet Dent 1970;23(4):441–8. Crossref
-
Fernandes RP, Quimby A, Salman S. Comprehensive reconstruction of mandibular defects with free fibula flaps and endosseous implants. J Diagn Treat Oral Maxillofac Pathol 2017;1(1):6–10. Crossref
-
Rude K, Thygesen TH, Sørensen JA. Reconstruction of the maxilla using a fibula graft and virtual planning techniques. BMJ Case Reports 2014;2014:bcr2014203601. Crossref
-
Linkow LI, Cherchève R. Theories and techniques of oral implantology. 1st ed. St. Louis: C. V. Mosby Co; 1970.
-
Dal Carlo L, Linkow L, Pasqualini M, Shulman M, Grivet Brancot L, Nardone M. Blade implants in the rehabilitation of severely atrophic ridges. Annals of Oral & Maxillofacial Surgery 2013;1(4):33. Crossref
-
Di Stefano DA, Iezzi G, Scarano A, Perrotti V, Piattelli A. Immediately loaded blade implant retrieved from a after a 20-year loading period: a histologic and histomorphometric case report. J Oral Implantol 2006;32(4):171–6. Crossref
-
Cappuccilli M, Conted M, Praissd ST. Placement and postmortem retrieval of a 28-year-old implant: a clinical and histologic report. J Am Dent Assoc 2004;135(3):324–9. Crossref
-
Dal Carlo L. Study over 7000 endosseous implants inserted during 25 years in 3300 interventions. Clinical results in different anatomical and functional situations. Statistical data and over 20 years iconographic documentation. J Dent Oral Health 2016;2(6):1–10.
-
Roberts RA. Types, uses, and evaluation of the plate-form implant. J Oral Implantol 1996;22(2):111–8.
-
Proussaefs P, Lozada J. Evaluation of two vitallium blade-form implants retrieved after 13 to 21 years of function: a clinical report. J Prosthet Dent 2002;87(2):412–5. Crossref
-
Mangano F, Bazzoli M, Tettamanti L, Farronato D, Maineri M, Macchi A, Mangano C. Custom-made, selective laser sintering (SLS) blade implants as a non-conventional solution for the prosthetic rehabilitation of extremely atrophied posterior mandible. Lasers Med Sci 2013;28(5):1241–7. Crossref
-
Rutkowski JL. Blade-form dental implants: FDA reclassification as a Class II dental implant device. J Oral Implantol 2013;39(6):633–4. Crossref
-
Farronato D, Fumagalli D, Asa’ad F, Pasini PM, Mangano F, Rasperini G. Failed blade implant after 25 years in function: case description and histologic analysis. Int J Periodontics Restorative Dent 2018;38(2):e29–e32. Crossref
-
Toti P, Barone A, Marconcini S, Menchini-Fabris GB, Martuscelli R, Covani U. Pose determination of a blade implant in three dimensions from a single two-dimensional radiograph. Dentomaxillofac Radiol 2018;47(4):20170258. Crossref
-
Sivolella S, Berengo M, Fiorot M, Mazzuchin M. Retrieval of blade implants with piezosurgery: two clinical cases. Minerva Stomatol 2007;56(1-2):53–61.
-
Stajčić Z, Stojčev Stajčić LJ, Kalanović M, Đinić A, Divekar N, Rodić M. Removal of dental implants: review of five different techniques. Int J Oral Maxillofac Surg 2016;45(5):641–8. Crossref
-
Noack N, Willer J, Hoffmann J. Long-term results after placement of dental implants: longitudinal study of 1,964 implants over 16 years. Int J Oral Maxillofac Implants 1999;14(5):748–55.
-
Strecha J, Jurkovic R, Siebert T, Prachar P, Bartakova S. Fixed bicortical screw and blade implants as a non-standard solution to an edentulous (toothless) mandible. Int J Oral Scien 2010;2:105–10. Crossref
-
Brägger U, Aeschlimann S, Bürgin W, Hämmerle CH, Lang NP. Biological and technical complications and failures with fixed partial dentures (FPD) on implants and teeth after four to five years of function. Clin Oral Implants Res 2001;12(1):26–34. Crossref
-
Cordaro L, Ercoli C, Rossini C, Torsello F, Feng C. Retrospective evaluation of complete-arch fixed partial dentures connecting teeth and implant abutments in patients with normal and reduced periodontal support. J Prosthet Dent 2005;94(4):313–20. Crossref
-
Nickenig HJ, Schäfer C, Spiekermann H. Survival and complication rates of combined tooth-implant- supported fixed partial dentures. Clin Oral Implants Res2006;17(5):506–11. Crossref
-
Davis SM, Plonka AB, Wang HL. Risks and benefits of connecting an implant and natural tooth. Implant Dent 2014;23(3):253–7. Crossref
-
Naert IE, Duyck JA, Hosny MM, et al. Freestanding and tooth-implant connected prostheses in the treatment of partially edentulous patients. Part I: an up to 15-years clinical evaluation. Clin Oral Implants Res. 2001;12:237–44.
-
Covani U, Marconcini S, Crespi R, Barone A. Immediate implant placement after removal of a failed implant: a clinical and histological case report. J Oral Implantol 2009;35(4):189–95. Crossref
CITING ARTICLES (1)
-
Kučera J, Lofaj F, Šimůnek A, Németh D. Finite element analysis of blade implants and their modifications as a nonstandard solution in toothless atrophied alveolar crest of mandible. Int J Dent Oral Health 2022;8(3): Crossref