
Infected Nasolabial Cyst
February 28, 2020
https://doi.org/10.23999/j.dtomp.2020.2.4
J Diagn Treat Oral Maxillofac Pathol 2020;4(2):38.
Under a Creative Commons license
HOW TO CITE THIS ARTICLE
Khadem AA. Infected nasolabial cyst. J Diagn Treat Oral Maxillofac Pathol 2020;4(2):38.
ARTICLE
A 33-year-old female presented to the dental clinic with complaints for rapid increasing (during last several days) of the painful edema in upper lip area and elevation of the left ala of the nose. Examination also revealed elevation of the nasal floor and a painful strictly demarcated oval shape fluctuated swelling (Panel A, arrows) underneath the mobile mucosa from the upper right central incisor to the upper left canine.
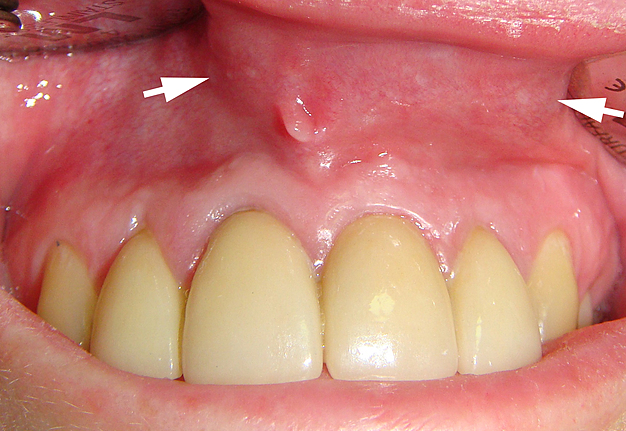

Panel A. Examination revealed elevation of the nasal floor and a painful strictly demarcated oval shape fluctuated swelling (arrows) underneath the mobile mucosa from the upper right central incisor to the upper left canine.
Cone-beam computed tomography (Panel B: panoramic view) showed no periradicular bony changes in the segment of anterior maxilla.
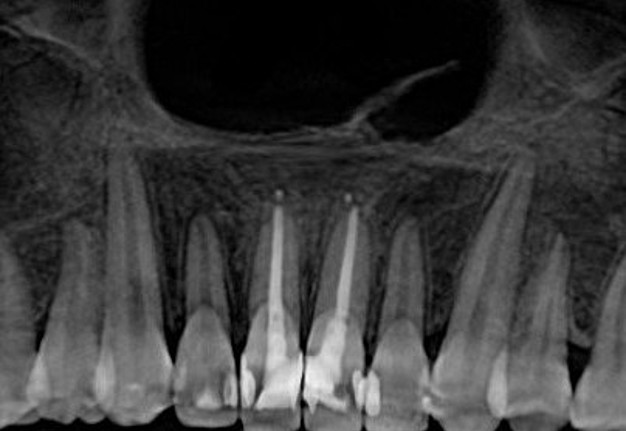
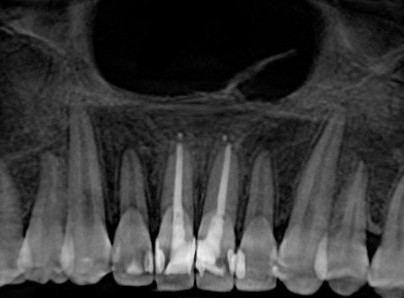
Panel B. Cone-beam computed tomography (panoramic view) showed no periradicular bony changes in the segment of anterior maxilla.
According to medical history the upper central incisors were endodontically treated several years ago due to the caries and pulpitis. Diagnosis of subperiosteal radicular/peripheral residual cyst was excluded and the diagnosis of infected nasolabial cyst (synonyms: developmental fissural cyst, nasal wing cyst) was established. The extraosseous cystic lesion was excised with intraoral approach under local anesthesia by Ievgen I. Fesenko, PhD 1 month after the treatment of cyst`s infected state. The histopathology confirmed the clinical diagnosis revealing an epithelial lining with a signs of fibrosis and inflammation of the cystic wall. 1-year followup showed no signs of recurrence. ■ DTJournal.org