
January 22, 2023
J Diagn Treat Oral Maxillofac Pathol 2023;7: 6–9.
doi: 10.23999/j.dtomp.2023.1.3
Under a Creative Commons license
HOW TO CITE THIS ARTICLE
Budihardja AS, Lius AA. The impact of the COVID-19 pandemic on primary cleft surgery. J Diagn Treat Oral Maxillofac Pathol 2023;7(1):6–9. https://doi.org/10.23999/j.dtomp.2023.1.3
NATIONAL REPOSITORY OF ACADEMIC TEXTS
https://nrat.ukrintei.ua/en/searchdoc/2023U000298/
ABSTRACT
Objective: The main objective of this study is to evaluate the early effects of the COVID-19 pandemic on primary cleft lip surgeries in a single high-volume center.
Material and Methods: A retrospective comparative cohort study of patients undergoing primary cleft lip and primary cleft palate repair before and during the pandemic was conducted. A sum of 194 patients, comprising of 100 patients taken pre-pandemic, and 94 patients who underwent primary cleft repairs during the pandemic were used in this study. The demographic factor and age groups were compared.
Results: Mean age of primary cleft repair was 6.1 ± 2.9 pre-pandemic (n = 66) and 6.9 ± 4.9 (n = 69) in the pandemic cohort (p = 0.229). The mean age at primary cleft palate repair was 22.3 ± 13.5 (n = 34) pre-pandemic and 23.6 ± 10.7 (n = 25) in the pandemic cohort (p = 0.7).
Conclusion: Primary cleft surgery was not significantly affected by the COVID-19 pandemic. Further studies are required to evaluate the psychological effects of the pandemic to patients and their families.
INTRODUCTION
COVID-19, or coronavirus disease, is defined as an infectious disease caused by the SARS-CoV-2 virus. People infected with this virus will typically develop mild to severe respiratory illness. In January 2020, the World Health Organization (WHO) declared COVID-19 a global health emergency, and on March 11, 2020, the WHO declared COVID-19 a global pandemic.1
In response to tackle the pandemic, countries across the world focused on increasing testing, amplifying PPE (personal protective equipment) supplies, ensuring adequate room and resources in hospitals, implementing health protocols to flatten the curve, and spread of disease, and stringent lockdown policies in some countries.
Hospitals implied a policy that elective and other non-essential surgeries are not done throughout the pandemic as PPE and care units in hospitals became too limited. On April 1, 2020, the American Cleft Palate Craniofacial Association (ACPA) released a statement declaring to delay primary cleft lip surgeries and take into consideration in prioritizing patient and doctor safety when considering whether to do a cleft lip repair2–4.
The ACPA also recommended to delay any non-urgent intraoral surgeries as such procedures impose risk to virus transmission.
These circumstances have undoubtedly affected cleft lip palate repair surgeries. Cleft lip repairs are typically done when a patient is 3-6 months old, while cleft palate repairs are done when a patient is 1-1.5 years old. This is a critical age to perform repairs because it reduces social stigma on the patients as well as enabling them to eat normally as well as assuring a better speech outcome.
The purpose of this study is to evaluate the early effects of the COVID-19 pandemic on primary cleft surgeries in a single high-volume center. The hypothesis of the study is that the COVID-19 pandemic will cause a delay in primary cleft surgeries.
MATERIAL AND METHODS
The type of study done was an analytic-comparative, categorical, uncoupled with a retrospective cohort design study. This study has been approved by the Faculty of Medicine University of Pelita Harapan ethical committee.
The population group of this study are patients undergoing primary cleft repair and primary cleft palate repair in Siloam Lippo Village Comprehensive Cleft Center, Tangerang, Indonesia. The pre-pandemic cohort included patients who underwent primary cleft lip/palate surgery from 2018-2019. The pandemic cohort included patients who underwent primary cleft lip/palate surgery from 2020-2021. Patients with syndromes and other congenital defects and submucosal cleft palates were excluded from this study.
During the COVID-19 pandemic, all patients admitted went through COVID-19 PCR test screening 2 days before surgery. Patient with positive PCR results is referred to pediatricians to receive further care.
Patient data was obtained from Siloam Hospital Lippo Village, Indonesia electronic medical record database. The data collected included patient demographic data, diagnosis, and type of surgery performed. Surgical delay is defined as the time deviation from standard protocol in the health institution to perform primary lip and primary palate repair surgery. In our health institute, primary lip surgery is done at age 3 months old, and primary palate surgery is done at 1 year old. Any surgical delay not caused by the COVID-19 outbreak is excluded from this study. Demographic data analysis was done using the Chi-square method, and patient age group variables during surgical intervention is tested with the unpaired T-test using SPSS version 26.0.
RESULTS
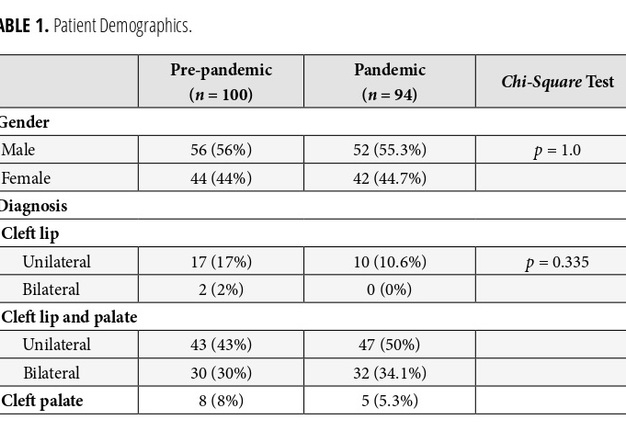
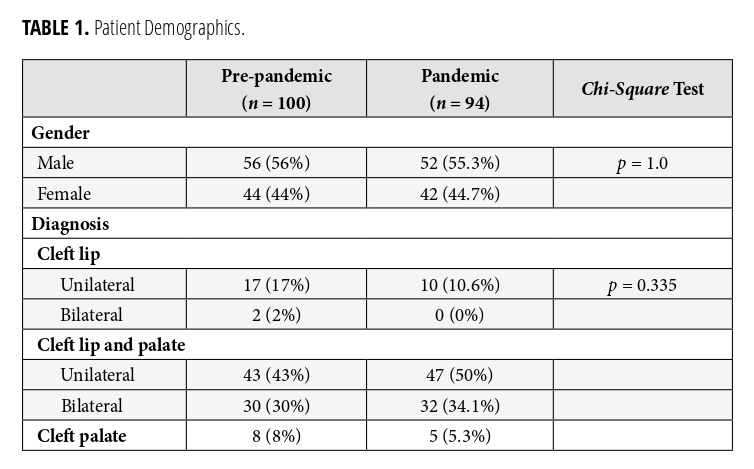
A total of 194 patients were involved in this study, of which 100 patients (51.5%) underwent primary cleft surgery before the COVID-19 pandemic, and 94 patients (48.5%) underwent surgery after the COVID-19 pandemic (Table 1). From the 194 patients in this study, 108 samples are male, and 86 samples are female. Based on type of cleft, 29 patients had a cleft lip (27 unilateral cleft lip and 2 bilateral cleft lip), 152 patients with cleft lip and palate (90 patients with unilateral cleft lip palate and 62 patients with bilateral cleft lip palate), and 13 patients with isolated cleft palate.
TABLE 1. Patient Demographics.
The 135 patients underwent primary cleft lip surgery, and 59 patients underwent primary cleft palate surgery.
Based on gender distinction, there were 56 (56%) male patients and 44 (44%) female patients in the pre-pandemic group, and 52 (55.3%) male patients and 42 (44.7%) female patients in the pandemic group. Demographic data analysis showed no significant difference between gender groups (p = 1.0).
Based on type of cleft, there were 17 (17%) patients with unilateral cleft lip, 2 (2%) patients with bilateral cleft lip, 43 (43%) patients with unilateral cleft lip palate, 30 (30%) patients with bilateral cleft lip palate, and 8 (8%) with isolated cleft palate in the pre-COVID 19-pandemic group. In the COVID-19 pandemic group, there were 10 (10.6%) patients with unilateral cleft lip, zero patients with bilateral cleft lip, 47 (50%) patients with unilateral cleft lip palate, 32 (34.1%) patients with bilateral cleft lip palate, and 5 (5.3%) patients with isolated cleft palate (Table 2). Data analysis using the Chi-square method showed no significant difference between the demographic data (p = 0.035).
TABLE 2. Comparison of Age at Surgical Intervention.
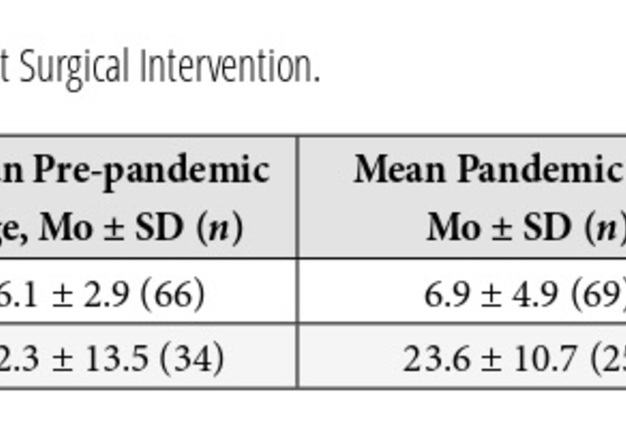
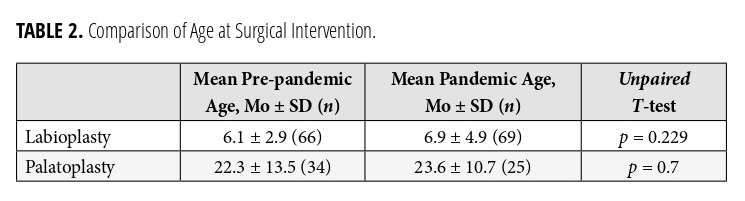
The mean age of primary cleft repair surgery was 6.1 ± 2.9 in the pre-pandemic (n = 66), and 6.9 ± 4.9 (n = 69) in the pandemic cohort (p = 0.229). The mean age of primary cleft palate repair surgery was 22.3 ± 13.5 (n = 34) in the pre-pandemic and 23.6 ± 10.7 (n = 25) in the pandemic cohort (p = 07). Six patients had surgery postponed due to COVID-19 infection.
DISCUSSION
The COVID-19 pandemic resulted in many elective and other non-essential surgical procedures to be deferred. This is mainly due to limited supply of masks and other personal protective equipment, as well as hospital in-patient care units. Despite a high demand, intraoral surgeries were particularly associated with a high virus transmission risk and therefore not recommended2,4.
Cleft lip palate repair surgeries were greatly affected by the COVID-19 pandemic in many countries around the world. The ACPA and other professional organizations strictly urged delaying all cleft surgeries. Primary cleft repairs are typically done when a patient is 3 months old if they met the standards of a minimal body weight of 5 kg and hemoglobin (Hb) level of 10. There is currently limited data on the negative implications of delaying primary cleft repairs.
Palatoplasty procedures should typically be done when a child is 1 year old in the bubbling phase. An intact palate can prevent regurgitation during feeding and allow velopharyngeal competence for better speech outcome. Delay closure of cleft palate will result in speech problem and hypernasality.
The results of this study were comparable with the results of similar studies conducted in other parts of the world: deferred primary cleft lip and primary cleft palate repair surgeries during the pandemic. Although there was no significant outcome, the psychological impacts to patients and their families must be considered, especially without knowing when the pandemic would end, and patients under the age of 5 not eligible to receive a COVID-19 vaccine.5–8
Other studies, such as the study done by Vander Burg and colleagues (2021) showed that in the period of January to December 2020, the number of cleft repair surgeries declined to as much as 25,444 cases.6 Patients are predominantly children and added to the number of 60,000 people left with untreated cleft lip palate. January to April 2020 showed the most significant decline in surgeries, while numbers then started to increase over May to December 2020.6
Managing cases of postponed cleft lip and palate became challenging for surgeons and hospitals. The psychosocial effects to patients and their families due to this delay requires close monitoring.
CONCLUSION
The COVID-19 pandemic noticeably impacted elective surgical procedures in hospitals. Although the number of surgeries plummeted during the beginning of the pandemic, numbers slowly started rising through the upcoming months as hospitals became more well equipped, personal protective equipment (PPE) became more readily available, and hospital staff adapted to the circumstances of the pandemic.
Further research is needed to better understand what factors affect surgeries during a pandemic, so that the healthcare system may be well equipped and prepared in the event of future disruption such as pandemics, wars, and/or natural disaster.
ETHICS APPROVAL
This study was conducted under the approval of Ethic Committee (No. 094/K-LKJ/ETIK/II/2022) Faculty of Medicine, University of Pelita Harapan, Tangerang, Indonesia.
CONFLICT OF INTEREST
The authors declare that there is no potential conflict of interest relevant to this article.
REFERENCES (8)
-
Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed 2020;91(1):157–60. Crossref
-
ACPA. ACPA statement on cleft lip/palate related surgeries and team care during the COVID-19 pandemic 2020. Published 2020. Available at: Link
-
COVIDSurg Collaborative. Elective surgery cancellations due to the COVID-19 pandemic: global predictive modelling to inform surgical recovery plans. Br J Surg 2020;107(11):1440–9. Crossref
-
Schoenbrunner A, Sarac B, Gosman A, Janis JE. Considerations for pediatric craniofacial surgeons during the COVID-19 outbreak. J Craniofac Surg 2020;31(6):e618–20. Crossref
-
Perry PR, Guttierrez AG. Cleft lip palate surgery during Covid-19 pandemic. Plast Reconstr Surg Global Open 2021;9(6):e3692. Crossref
-
Vander Burg R, Agrawal K, Desai P, Desalu I, Donkor P. Impact of COVID-19 on elective cleft surgery in low- and middle-income countries. Plast Reconstr Surg Global Open 2021;9(6):e3656. Crossref
-
Bruce MK, Pfaff MJ, Anstadt EE, Losee JE, Goldstein JA. The impact of the covid-19 pandemic on cleft care. Plast Reconstr Surg Global Open 2021;9(4):e3587. Crossref
-
Ferry AM, Beh HZ, Dibbs RP, Davies LW, Xue AS, Dempsey RF, Olorunnipa S, Maricevich RS, Monson LA, Rodgers A, Wirthlin JO, Hollier LHJr, Buchanan EP. Impact of COVID-19 on cleft surgical care. FACE 2021;2(1):6–12. Crossref