
December 28, 2017
https://doi.org/10.23999/j.dtomp.2017.3-4.9
J Diagn Treat Oral Maxillofac Pathol 2017;1:164−7.
Under a Creative Commons license
How to cite this article
Ushko NO. Correction of lysozyme content in mixed saliva in patients with jaw ameloblastomas. J Diagn Treat Oral Maxillofac Pathol 2017;1(3−4):164−7.
Contents: Abstract | Introduction | Matherial and Methods | Results | Conclusion | Funding | Conflict of Interest | Role of Co-Authors | Ethical Approval | Patient Consent | Acknowledgemets | References (14)
ABSTRACT
Purpose: Determine the content of lysozyme in mixed saliva in patients with ameloblastomas of the jaws in the dynamics of the treatment, as well as the effectiveness of using the drug Lysobact for immunocorrection.
Material and Methods: 31 patients with ameloblastomas of the jaws were examined in the dynamics of the treatment and in the rehabilitation period.
Results: A decrease in local non-specific resistance of the body (studied by the content of lysozyme in mixed saliva) in patients with jaw ameloblastomas during hospitalization and after surgical treatment was established. The purpose of the drug Lysobact allowed normalizing the level of lysozyme content in the mixed saliva of these patients in the rehabilitation period.
Conclusions: The use of the drug Lysobact for 2 weeks in patients with ameloblastomas of the jaws allows to completely normalizing the local nonspecific resistance of the organism and significantly reduces the number of inflammatory complications.
Introduction
Based on the examination of patients with ameloblastomas of the jaws, the secretion of mixed saliva (oral fluid), the saliva of large salivary glands (parotid and submandibular), as well as the number and functional activity of small salivary glands, significantly decreased in comparison with healthy people after surgical treatment. Normalization of saliva secretion, which is secreted by large and small salivary glands, occurs not earlier than 2-3 weeks after gentle resection of the lower jaw and 2 months after the classical resection (with violation of bone continuity). This fact indicates that in patients with ameloblastomas in the postoperative period [1-4], the local protective factors of the organism appear to decrease, which leads to the development of inflammatory processes from the mucous membrane of the oral cavity.
To correct the local nonspecific resistance of the body, which is regulated by the level of lysozyme in mixed saliva, there are a lot of medications in the arsenal of the doctor. We were interested in medications that would be as close to the natural components of the human body as possible. Lysozyme. Thus, our attention was drawn to the drug Lysobact.
"Lysobact©" (Bosnalijek d.d., Sarajevo, Bosnia and Herzegovina) approved by the order of the Ministry of Health of Ukraine on March 14, 2005, No. 106 (registration certificate No. UA/2790/01/01). The drug is produced in blisters of 10 tablets, which are used for resorption. One tablet contains 20 mg of lysozyme chloride and 10 mg of pyridoxine hydrochloride. It is known that lysozyme is a mucopolysaccharide effective against gram-positive and gram-negative bacteria (the insoluble polysaccharides of the cell wall of the microbe are transformed into soluble mucopeptides), and also effective against fungi and viruses. Lysozyme exhibits local anti-inflammatory activity and increases the nonspecific resistance of the body. Pyridoxine (vitamin B6) provides a protective effect on the mucosa of the oral cavity, preventing the development of thrush. Scheme of drug usage: adults take 2 tablets (dissolve) 3─4 times a day for 14 days. Contraindication to the use of Lysobact is an increased sensitivity to the components of the drug.
The purpose of the study was to determine the level of lysozyme in mixed saliva of patients with ameloblastomas before surgical treatment (Fig 1), in the dynamics of the postoperative period, and to establish the effectiveness of using the drug Lysobact for immunocorrection.


FIGURE 1A. An extraoral (A) and intraoral (B) appearance of follicular ameloblastoma of the right mandible in 57-year-old lady. The patient is noted the tumor growth during last 30 years. On the intraoral image (B) and panoramic x-ray (C) the tumor is indicated by arrows.
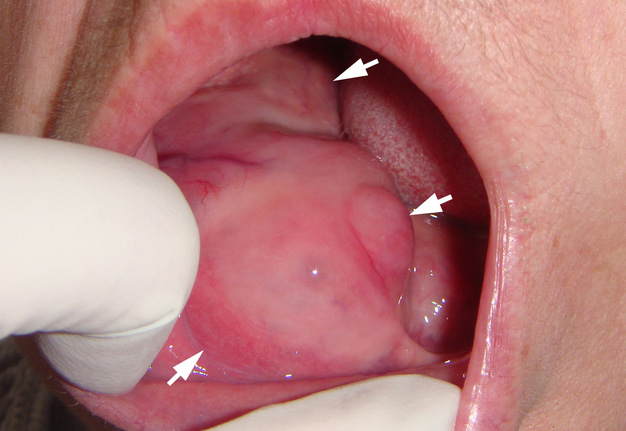
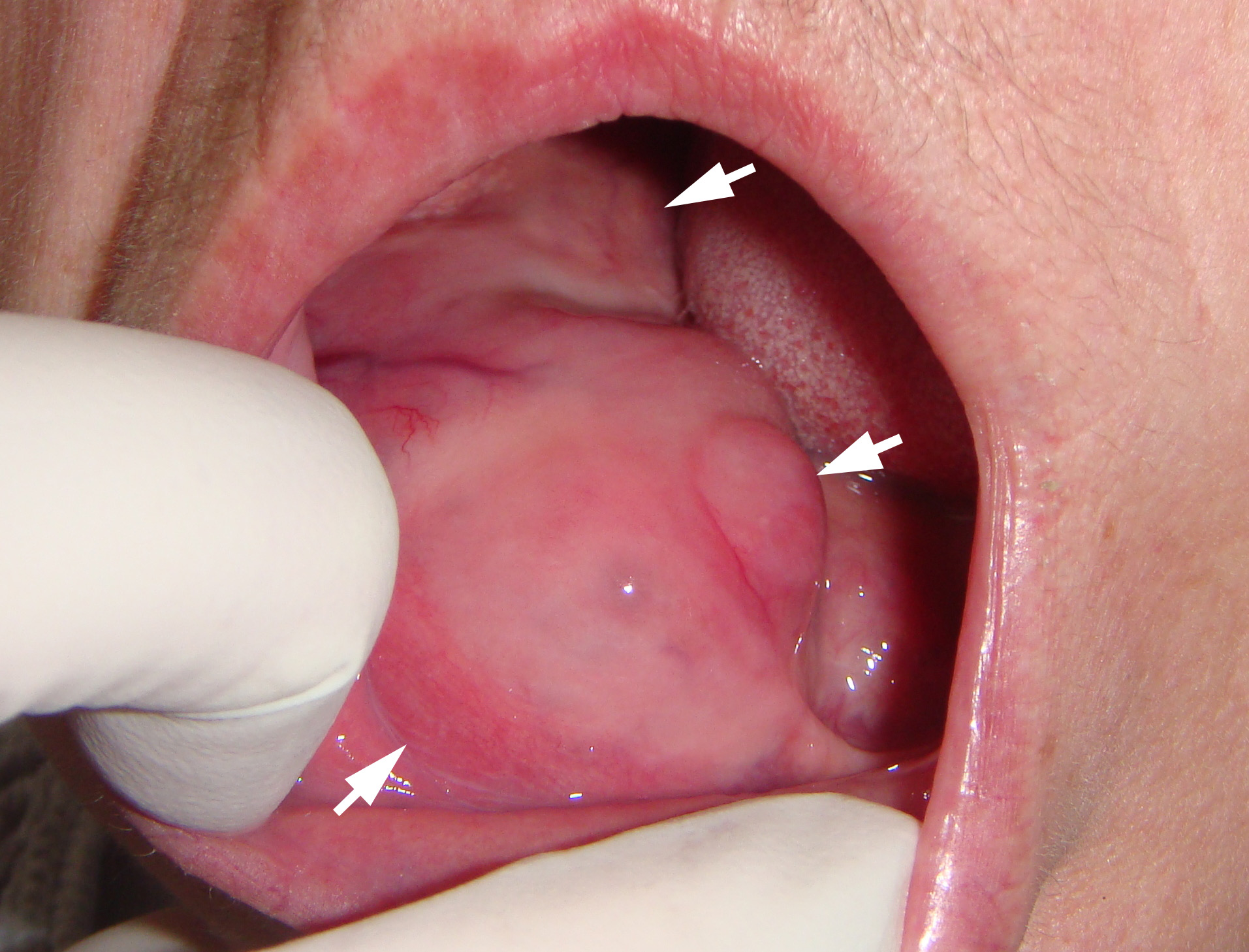
FIGURE 1B. An extraoral (A) and intraoral (B) appearance of follicular ameloblastoma of the right mandible in 57-year-old lady. The patient is noted the tumor growth during last 30 years. On the intraoral image (B) and panoramic x-ray (C) the tumor is indicated by arrows.
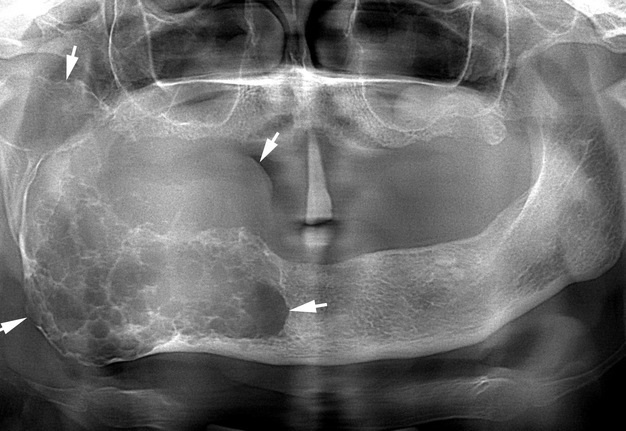
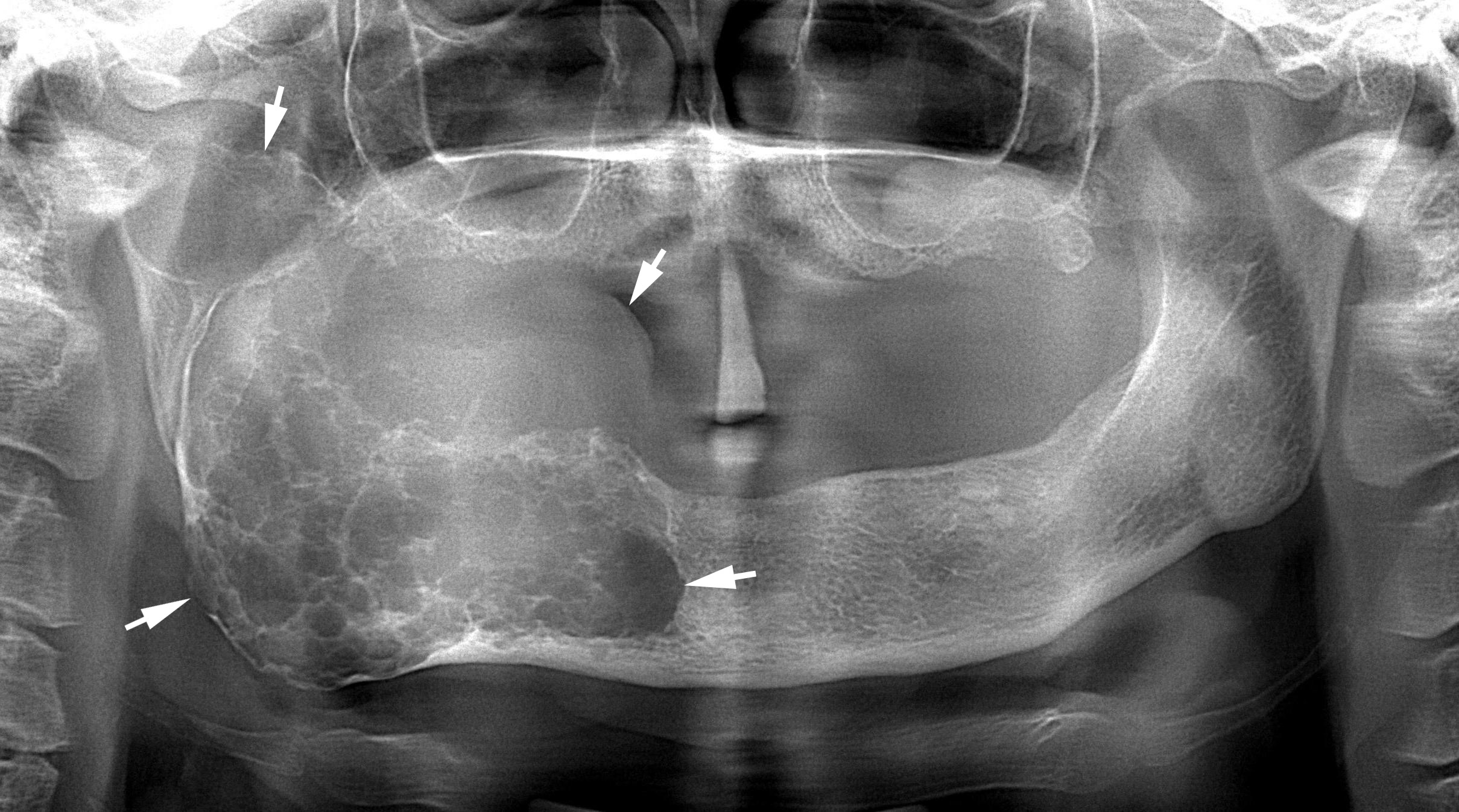
FIGURE 1C. An extraoral (A) and intraoral (B) appearance of follicular ameloblastoma of the right mandible in 57-year-old lady. The patient is noted the tumor growth during last 30 years. On the intraoral image (B) and panoramic x-ray (C) the tumor is indicated by arrows.
Materials and Methods
31 patients with ameloblastomas of jaws aged from 24 to 59 years were examined. Patients were examined at hospitalization, 5─7 and 14─17 days after surgery, 7─8 days and 16─18 days after the start of treatment with the drug Lysobact, and also 2─2.5 months after the performed operation.
All patients were assessed the level of lysozyme in mixed saliva (oral fluid). The following saliva collection conditions were applied: saliva was collected on an empty stomach, the patient collected saliva in the mouth for 1 minute, then spit it into a special container. The concentration of lysozyme in the investigated material was determined by the method of Motavkina (1979) [5].
In addition to the previously mentioned drug Lysobact, patients in the postoperative period underwent symptomatic treatment (using anesthetics, hygienic oral care, etc.).
The control group consisted of 29 practically healthy people (without concomitant diseases) with a sanitized oral cavity.
All the data obtained in the course of the study are processed mathematically using the Student test. The parameters were considered reliable at p<0.05.
Results
The results of the examination of 31 patients showed (Table 1) that when the patients with ameloblastoma were hospitalized, the content of lysozyme in mixed saliva (oral fluid) was 0.016 ± 0.001 g/l (p<0.001), which indicated a significant decrease in its level in comparison with the control group, healthy people (0.023 ± 0.001 g/l). Five to seven days after the operation, the content of lysozyme in mixed saliva decreased even more than in the previous study period (hospitalization), as well as in the control group, and was 0.012 ± 0.001 g/l (p<0.001). 14─17 days after surgery, the content of lysozyme in mixed saliva continued to decrease and already significantly differed not only in comparison with healthy people, but also in comparison with the previous survey period (5─7 days after the surgery). Attention is drawn to the fact that the more difficult the operation was, the lower the lysozyme levels in the mixed saliva. The lowest levels of lysozyme content in mixed saliva were found in patients after classical lower jaw resection, and less pronounced ─ after excisional biopsy and gentle resection of the mandible.
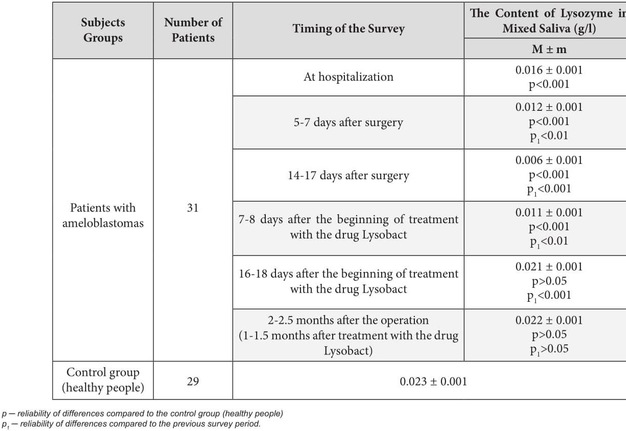
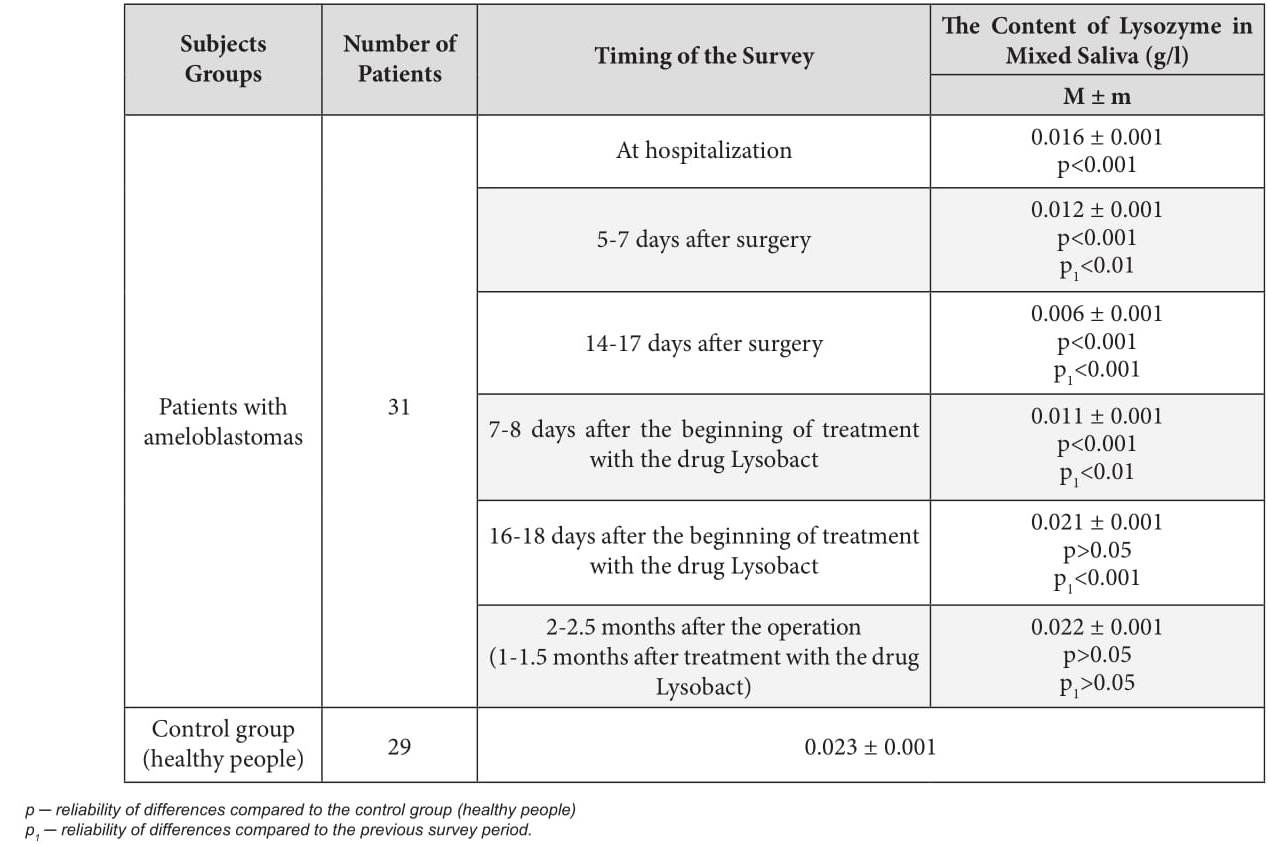
TABLE 1. The content of lysozyme in mixed saliva in patients with ameloblastoma in the dynamics of the treatment
Thus, on the basis of the conducted examination of patients with ameloblastomas of the jaws, it was found that when they were hospitalized, the content of lysozyme in the mixed saliva was already significantly lower in them than in healthy people. After 5-7 days after the operation, the content of lysozyme in mixed saliva was even greater and significantly decreased, and after 14─17 days after the surgical intervention (at discharge of the patients from the hospital) the level of lysozyme reached the lowest values. A significant decrease in the level of lysozyme in mixed saliva in this period of the survey indicated a decrease in local nonspecific resistance of the organism not only during hospitalization (in the presence of this tumor in the oral cavity), but also in the postoperative period. This was evidenced by an increase in the number of inflammatory manifestations from the mucous membrane of the oral cavity from 46.7% (when hospitalized) to 96.7% (when discharging from the hospital).
As a result of examination of 31 patients in the rehabilitation period, after the operative intervention, we found that the level of lysozyme in mixed saliva on the 7th─8th day after the use of the drug Lysobact significantly increased in comparison with the previous period of the examination (when the patient was discharged from the hospital), but still remained 2 times lower than normal and was 0.011 ± 0.001 g/l (p<0.001). This indicated the preservation of a low level of local nonspecific resistance of the organism in these patients (Table 1). Therefore, the treatment of patients with this drug, we continued in the previous dosages.
16─18 days after the beginning of treatment with the drug Lysobact, the content of lysozyme in mixed saliva significantly increased in comparison with the previous period of the examination and practically did not differ from the group of healthy people. The content of lysozyme in mixed saliva on the 16─18 day after the appointment of this drug was 0.021 ± 0.001 g/l (p>0.05). At this stage, the use of the drug Lysobact was completed. Thus, the duration of the drug Lysobact was 14 days (2 weeks).
To determine the level of lysozyme in mixed saliva, we conducted another, final, examination of previously treated patients 2─2.5 months after the surgery (1─1.5 months after the end of treatment with the drug Lysobact). It was established that the content of lysozyme in mixed saliva in this period was not significantly different from the control group of observation (healthy people) and was 0.023 ± 0.001 g/l (p>0.05). In the oral cavity of these patients, we did not reveal any inflammatory complications from the oral mucosa.
Conclusion
Based on the conducted examinations of patients with ameloblastomas of the jaws [6-14], it was found that the content of lysozyme in the mixed saliva of patients during hospitalization was significantly lower than normal, and after surgery it was further reduced.
To correct the local nonspecific resistance of the body, we applied the drug Lysobact. The drug Lysobact was prescribed for 14 days (2 weeks). After 16─18 days after the start of treatment with this drug, the content of lysozyme in mixed saliva was normalized and preserved in a remote postoperative period.
Funding
None.
Conflict of Interests
None.
Role of Author
Natalia O. Ushko (concept of the paper, material collection, and writing)
Ethical Approval
Approval was obtained from the Medical Ethics Committee of the Shupyk National Medical Academy of Postgraduate Education, Kyiv, Ukraine.
Patient Consent
Written patient consent was obtained to publish the clinical images.
Acknowledgements
High quality image C of Figure 1 is courtesy of Nadia I. Paterega, PhD Student, Lviv, Ukraine; Image A and B of Figure 1 is courtesy of Ievgen I. Fesenko, Assіs Prof; Kyiv, Ukraine.
References (14)
-
Tymofieiev OO. Manual of maxillofacial and oral surgery [Russian]. 5th ed. Kyiv: Chervona Ruta-Turs; 2012.
-
Fernandes RP, Quimby A, Salman S. Comprehensive reconstruction of mandibular defects with free fibula flaps and endosseous implants. J Diagn Treat Oral Maxillofac Pathol 2017;1(1):6−10.
-
Qaisi M, Kolodney H, Swedenburg G, et al. Fibula jaw in a day: state of the art in maxillofacial reconstruction. J Oral Maxillofac Surg 2016;74(6):1284.e1-1284.e15.
-
Tymofieiev OO. Maxillofacial surgery [Russian]. 2nd ed. Kyiv: Medytsyna; 2015.
-
Motavkina NS, Kovalev VM, Sharonov AS. Micromethod of quantitative determination of lysozyme [Russian]. Laboratornoye delo 1979;12:722–4.
-
Chukwuneke FN, Anyanechi CE, Akpeh JO, et al. Clinical characteristics and presentation of ameloblastomas: an 8-year retrospective study of 240 cases in Eastern Nigeria. Br J Oral Maxillofac Surg 2016;54(4):384−7.
-
Tymofieiev OO, Ushko NO, Vesova OP, Yarifa MO. Diagnostics of severity of the trigeminal nerve injuries during jaws surgeries. J Diagn Treat Oral Maxillofac Pathol 2017;1:32−9.
-
Tymofieiev OO, Ushko NO, Vesova OP, Yarifa MO. Treatment of postoperative neuropathy of the trigeminal nerve. J Diagn Treat Oral Maxillofac Pathol 2017;1:113−22.
-
Hammarfjord O, Roslund J, Abrahamsson P, et al. Surgical treatment of recurring ameloblastoma, are there options? Br J Oral Maxillofac Surg 2013;51(8):762−6.
-
Tymofieiev OO, Ushko NO, Tymofieiev OO, Yarifa MO, Fesenko IeI. Prevention of inflammatory complications upon surgeries in maxillofacial region. J Diagn Treat Oral Maxillofac Pathol 2017;1:105−12.
-
Chernushenko YeF, Kogosova LS. Immunological researches in clinic [Russian]. Kyiv: Zdorov'ya; 1978.
-
Tymofieiev OO. Essentials of maxillofacial surgery [Russian]. 1st ed. Moskow: Meditsinskoye Informatsionnoye Agentstvo; 2007.
-
Bansal S, Desai RS, Shirsat P, et al. The occurrence and pattern of ameloblastoma in children and adolescents: an Indian institutional study of 41 years and review of the literature. Int J Oral Maxillofac Surg. 2015;44(6):725−31.
-
Tymofieiev OO. Maxillofacial surgery [Ukrainian]. 2nd ed. Kyiv: Medytsyna; 2017.