
Extensive and Advanced Craniofacial Dysplasia
December 13, 2022
J Diagn Treat Oral Maxillofac Pathol 2022;6: 158–60.
Under a Creative Commons license
HOW TO CITE THIS ARTICLE
Grimaldi Finol GA, Hawamdeh S, Al Khalil M. Extensive and advanced craniofacial dysplasia. J Diagn Treat Oral Maxillofac Pathol 2022;6(12):158–60. https://doi.org/10.23999/j.dtomp.2022.12.2
NATIONAL REPOSITORY OF ACADEMIC TEXTS
https://nrat.ukrintei.ua/en/searchdoc/2022U000202/
Article


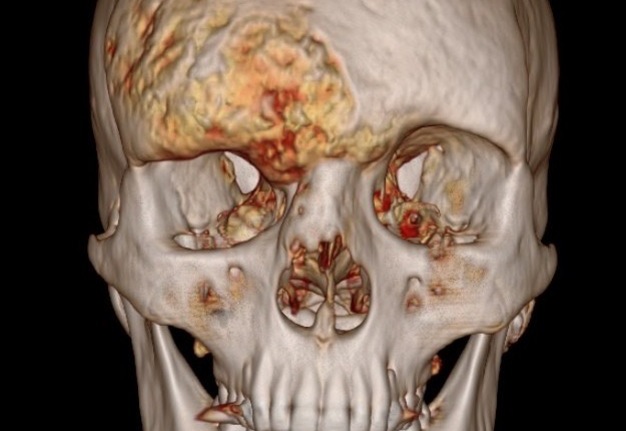
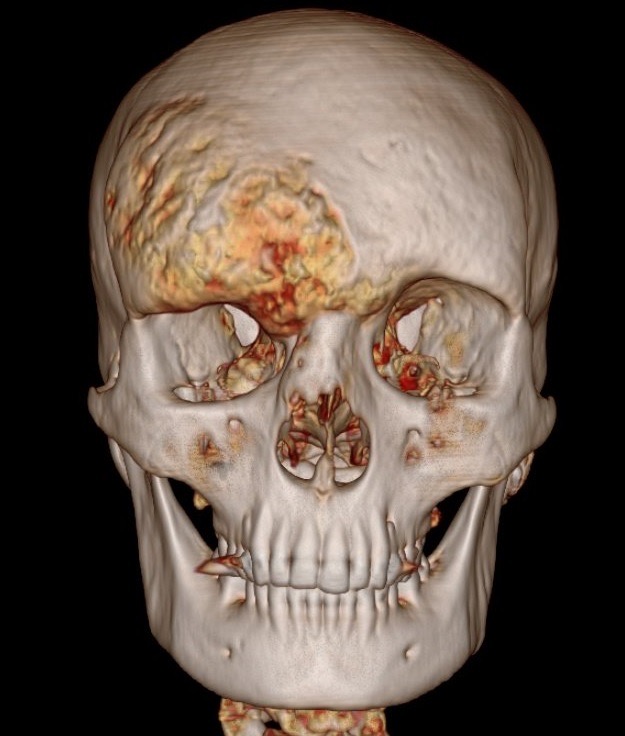
PANEL A.


PANEL B.
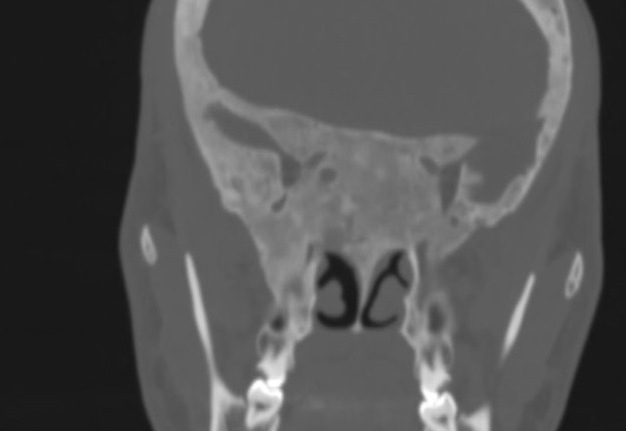
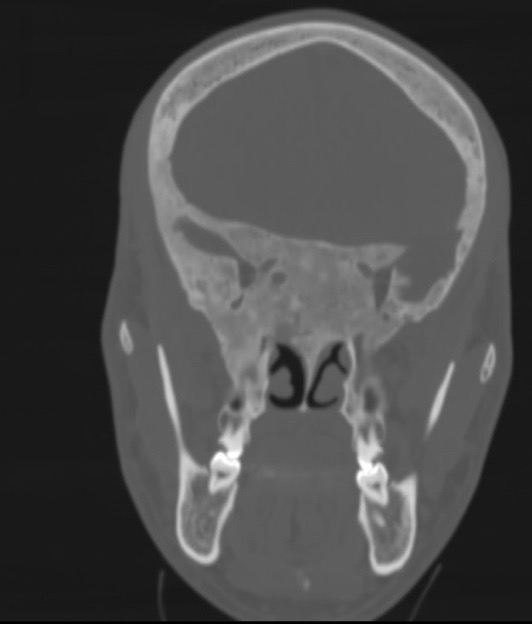
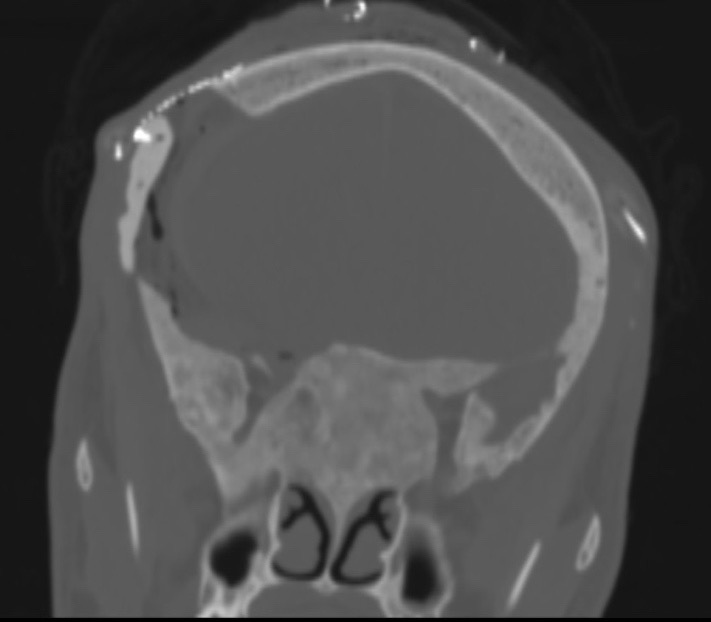
PANEL C.
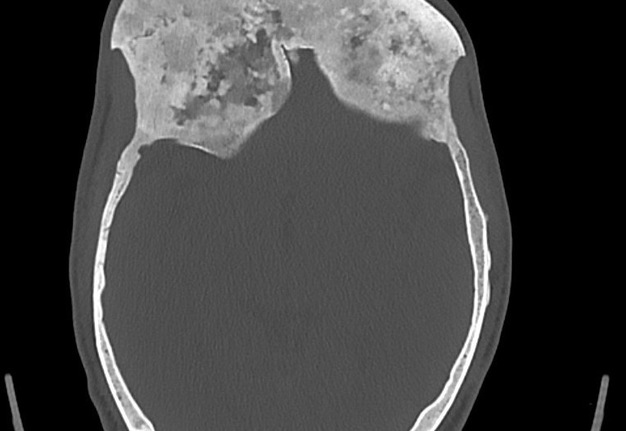
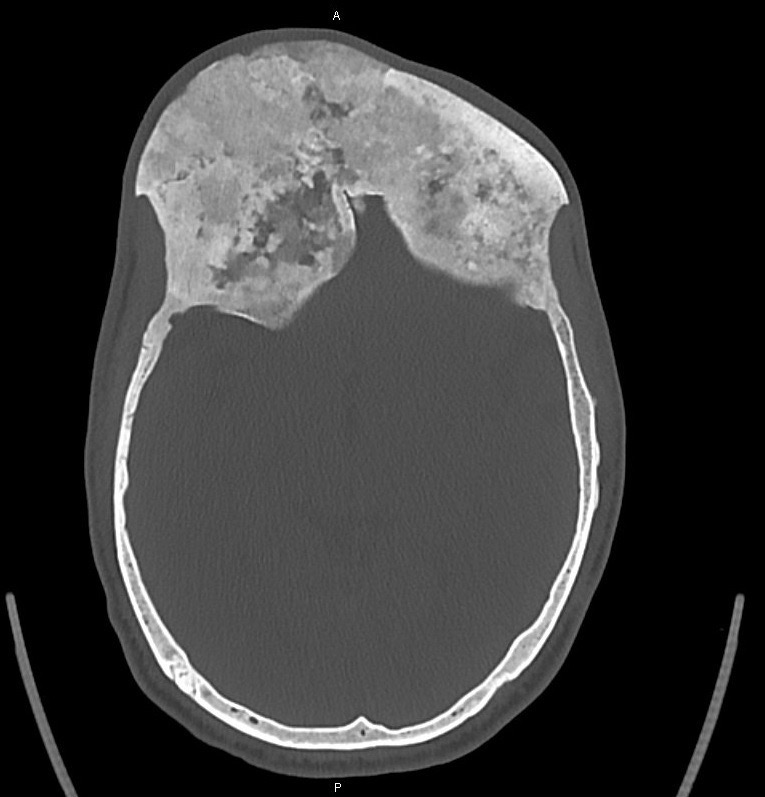
PANEL D.

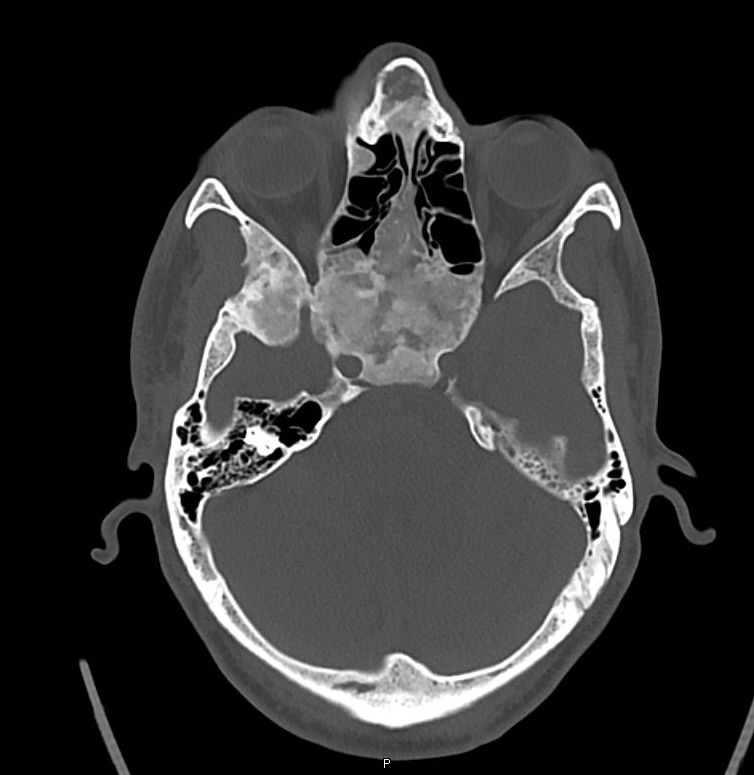
PANEL E.
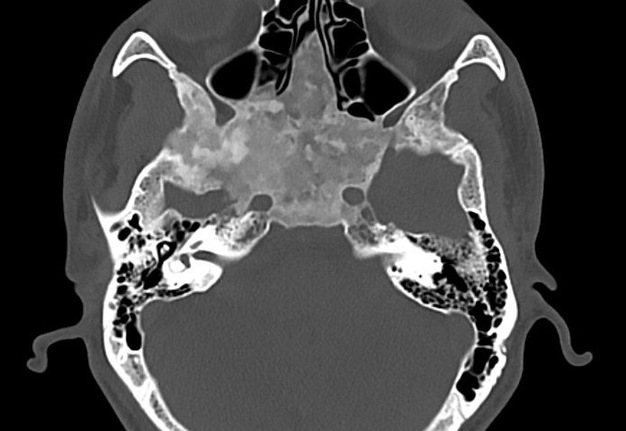

PANEL F.
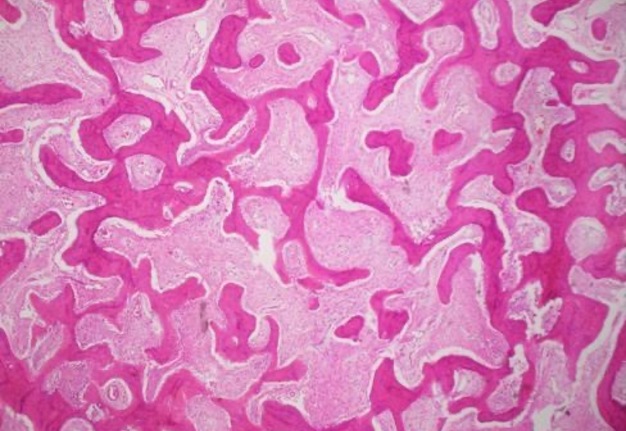

PANEL G.
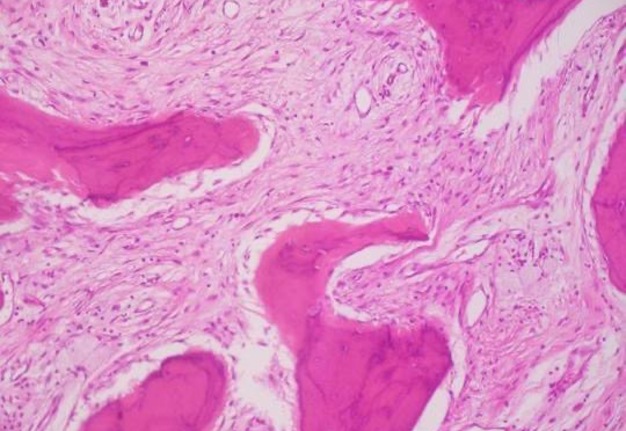
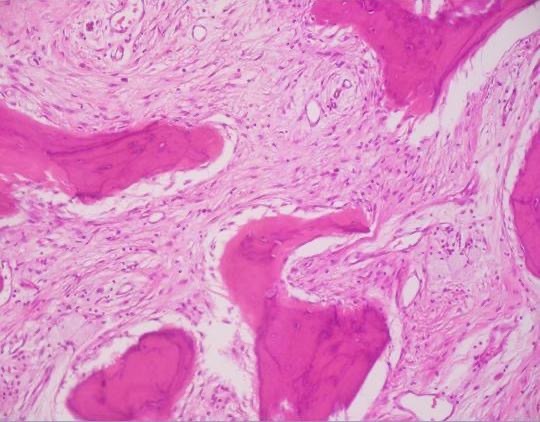
PANEL H.


PANEL I.
PANEL J.

PANEL K.
Download PANEL A–K in one file (1.85 mb).
A 35-year-old Syrian patient presented to our department complaining of 7-year history of asymptomatic hard swelling in right side of the frontotemporal and naso-orbito-ethmoidal region, reaching the contralateral side (Panel A and B). Patient stated that from 1 year back his visual acuity has been decreased compared with the previous 6 years. Computed tomography (CT) with contrast (Panel C–F) showed diffuse bony expansion involving the frontal bones bilaterally. Bone expansion was more on the right side extending into the vertical plates as well as the horizontal plates forming the roof extending to involve the cribriform plates and into the crista galli extending posteriorly to involve the sphenoid bone including the body, greater and lesser wings of the sphenoid bone as well as the clinoid processes ends extending to the roots of the pterygoid plates. Multidisciplinary decision team meeting was done, with neurosurgery, anesthesiology, and maxillofacial surgery to decide the treatment. Under the general anesthesia the patient underwent remodeling and recontouring of the facial and cranial bones through bilateral occipital approach. Using the unilateral frontotemporal extradural approach and retracting the dura and reaching the base of the skull the anterior clinoidectomy for optic nerve decompression was performed. Right clinoid process surgery reshaped the base of the skull releasing the bone which compressed the right orbital nerve. Affected bone which involved the frontotemporal area was removed and reconstruction was performed with cranioplasty fixed with osteosynthesis to the adjacent and healthy bony structures. The resected bone was submitted to Hamad general hospital histopathology laboratory which reported following fixation and decalcification irregular shaped trabeculae of immature woven bone scattered in a loosely hypercellular stroma histopathological diagnosed as fibrous dysplasia (Panel G and H: Hematoxilyn and eosin staining). After 5 days of medical management as inpatient, the patient was discharge with close follow up. Patient was followed up in a weekly basis with a normal postoperative status. 5 months after the surgery (Panel I, photography on postoperative day 120 showed remanent dystopia but generalized acceptable craniofacial projection), patient stated to have improvement in his visual acuity compared to his base line as well as craniofacial projection with a remanent vertical dystopia. Panel J and K compare preoperative CT (Panel J) where anterior clinoid process involved with the pathology is noted and postoperative CT (Panel K) which reveals removal of anterior clinoid process for orbital nerve decompression. ■ DTJournal.org