
Rehabilitation of a Patient with Cerebro-Costo-Mandibular Syndrome Using a Hybrid Digital-Analog Workflow and CAD-CAM Subperiosteal Implant System
Received 31 January 2026
Revised 17 March 2026
Accepted 24 March 2026
Published online 25 March 2026
J Diagn Treat Oral Maxillofac Pathol 2026; 10: 100316.
DOI: https://doi.org/10.23999/j.dtomp.2026.3.100316
Under a Creative Commons license (CC BY-NC-SA 4.0)
HOW TO CITE THIS ARTICLE: AMA STYLE
AlBaghli A, Wun E, Powell K, Ponto J, Kase MT. Rehabilitation of a patient with cerebro-costo-mandibular syndrome using a hybrid digital-analog workflow and CAD-CAM subperiosteal implant system. J Diagn Treat Oral Maxillofac Pathol. 2026;10(3):100316. doi:10.23999/j.dtomp.2026.3.100316

ABSTRACT
Rehabilitation of patients with cerebro-costo-mandibular syndrome (CCMS) and severe trismus presents unique challenges, as conventional impression and intraoral scanning techniques are often not feasible. This case report describes the successful use of a combined digital-analog workflow to fabricate a definitive mandibular full-arch monolithic zirconia prosthesis on a KLS Martin IPS® patient-specific subperiosteal framework. The treatment was selected as an alternative to more aggressive options such as mandibulectomy with free tissue transfer reconstruction with endosseous implants, or additional bone distraction osteogenesis (DO), which was not feasible due to severe mandibular-cranial angulation that prevented proper occlusal plane establishment. Placement of a subperiosteal implant enabled the metal substructure to rest directly on the mandible while multiunit abutments emerged into the oral cavity, leveling the occlusal plane to match the maxillary arch. During the process of collecting records and restoring the mandibular arch, a back-pour cast was fabricated from the provisional prototype and digitized, followed by stereolithography scanning of the cast and extraoral photogrammetry using the ICam4D system [14]. Implant positions were captured with sub-5 um accuracy, and occlusal records were collected after scanning the critical zones of the antagonist followed by reseating the prototype intraorally and scanning the bite. The final prosthesis demonstrated a passive fit with excellent function and esthetics. This approach highlights the value of integrating photogrammetry and cast digitization in cases with limited intraoral access, offering a predictable and reproducible method for complex rehabilitations.
Clinical Significance
This case highlights the integration of modern digital design and surgical technology in the rehabilitation of a patient with cerebro-costo-mandibular syndrome (CCMS), a rare congenital disorder that is characterized by severe mandibular hypoplasia and rib anomalies.
Conventional reconstructive approaches often fail to achieve adequate mandibular form or bone volume in syndromicpatients [15]. The use of a patient specific computer-aided design and computer-aided manufacturing (CAD-CAM) titanium subperiosteal implant enabled functional mandibular reconstruction without the morbidity associated with vascularized bone grafting, especially in the case of a younger patient as described.
By combining precise digital surgical planning with ICam photogrammetry and a cast digitization workflow, this approach demonstrates how customized subperiosteal frameworks can restore mandibular form, function, and esthetics inpatients once considered non-restorable using traditional methods.
INTRODUCTION
Cerebro-costo-mandibular syndrome (CCMS) is a rare congenital disorder first described by Smith and colleagues in 1966 [1]. It is characterized by mandibular hypoplasia, glossoptosis, and posterior rib defects, often leading to neonatal respiratory compromise. Fewer than 100 cases have been documented [2, 3], with most infants presenting with micrognathia, feeding difficulties, and some degree of airway obstruction. Mandibular hypoplasia is the most critical craniofacial feature, directly contributing to airway compromise. Initial management strategies range from positioning and airway adjuncts to tracheostomy [4], but these are invasive and can impact quality of life.
Mandibular distraction osteogenesis (DO) emerged as a preferred approach to manage airway obstruction [5-7], allowing gradual lengthening of bone and soft tissue to improve function and avoid tracheostomy. Despite its effectiveness, long-term outcomes are less predictable [6, 7], especially in syndromic patients who may continue to exhibit mandibular deficiency. Dental complications and growth limitations often preclude conventional endosseous implant placement.
Historically, subperiosteal implants were associated with high complication rates. However, advances in computer-aided design and computer-aided manufacturing (CAD-CAM) technology [8], cone beam computed tomography (CBCT)-based design, and rigid fixation with multiple mini-screws have improved outcomes substantially. Pure titanium frameworks allow for osteointegration, unlike older cobalt-chromium frameworks. In cases of severe mandibular hypoplasia or atrophy, CAD-CAM subperiosteal implants provide a realistic path for rehabilitation. When combined with digital-analog workflows such as extraoral photogrammetry (ICam4D; Imetric 4D Imaging Sàrl) and cast digitization, clinicians can capture implant and occlusal records reliably even when intraoral access is severely restricted.
CASE DESCRIPTION
Patient Information
A 21-year-old male with CCMS presented with complete mandibular edentulism, severe mandibular atrophy, and limited oral opening. Retained maxillary dentition was present.
He originally underwent bilateral mandibular DO at the age of two years for airway obstruction. Persistent mandibular hypoplasia into adulthood required a repeat DO at age 19, achieving approximately 18-23 mm advancement at 1 mm/day. As reported in syndromic craniofacial literature, long-term mandibular form after distraction can remain suboptimal due to altered growth vectors and limited intrinsic regenerative capacity [6-8, 15]. Postoperative imaging demonstrated inadequate mandibular width and incomplete consolidation (Fig 1).
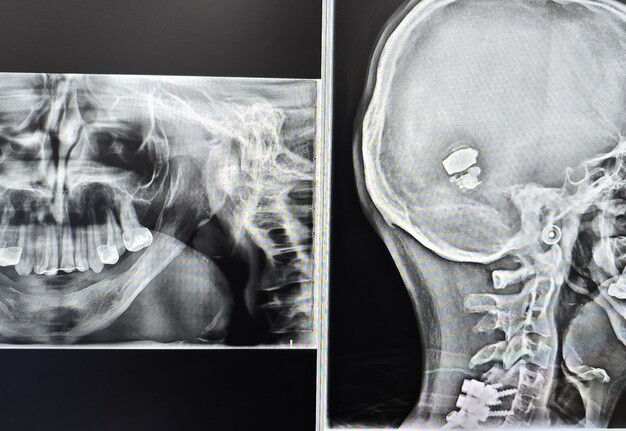
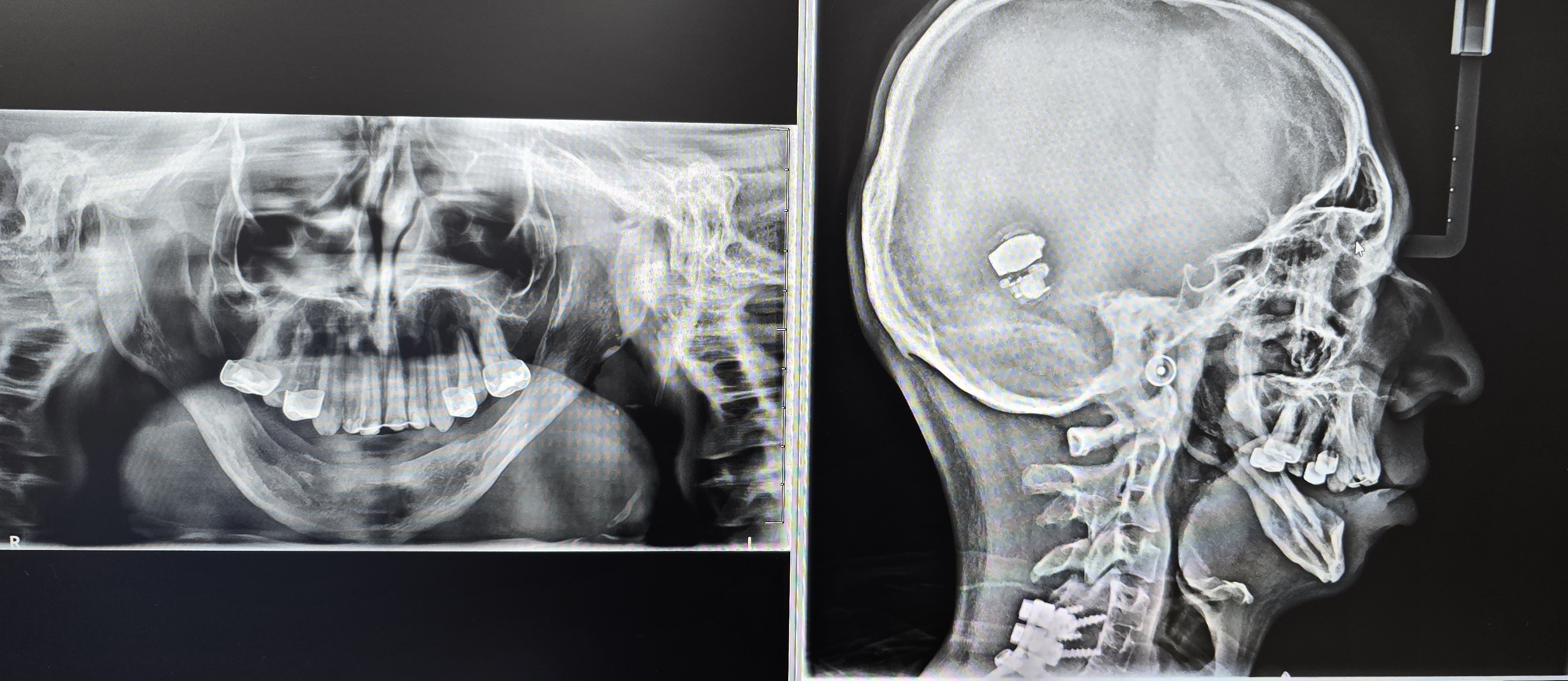
FIGURE 1. Pre-treatment panoramic and lateral cephalometric radiographs demonstrating the characteristic mandibular hypoplasia and facial profile associated with cerebro-costo-mandibular syndrome.
Following his second DO and due to persistent a thin mandibular alveolar ridge, bone morphogenetic protein (BMP)-augmented allograft reconstruction was attempted about half a year later but failed to generate sufficient bone volume. This finding is consistent with reports of variable graft success in congenital mandibular deficiency [16]. Given two prior distraction attempts, graft failure, and the morbidity associated with fibula free-flap mandibular reconstruction, a CAD-CAM titanium subperiosteal implant was selected as definitive treatment. Patient has agreed to the proposed treatment and has signed consent form also for documentation and publication of his case.
Definitive Subperiosteal Implant Procedure
Records for this patient were collected using a dual-scan CBCT and intraoral scanning. A surgical planning session was completed with KLS Martin for the fabrication of a CAD-CAM subperiosteal implant system with immediate loading of a mandibular prototype (Figs 2-5).
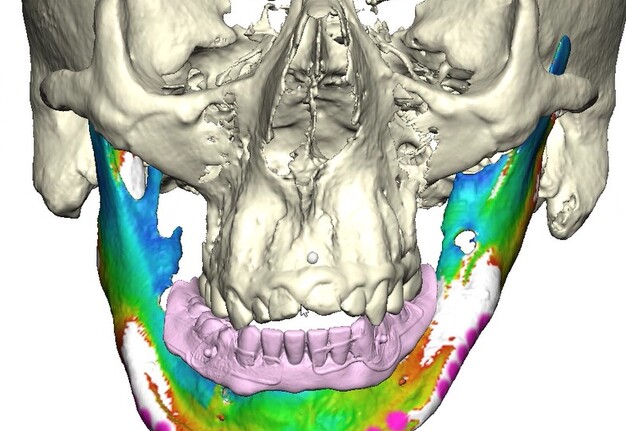
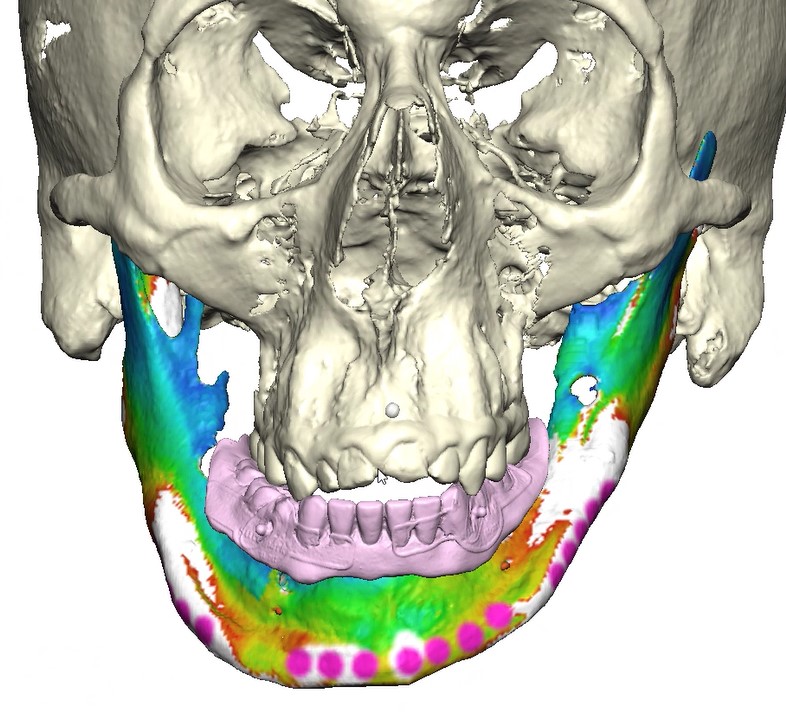
FIGURE 2. Virtual surgical planning (VSP) session with KLS Martin for the mandibular subperiosteal implant system with prototype, frontal view.
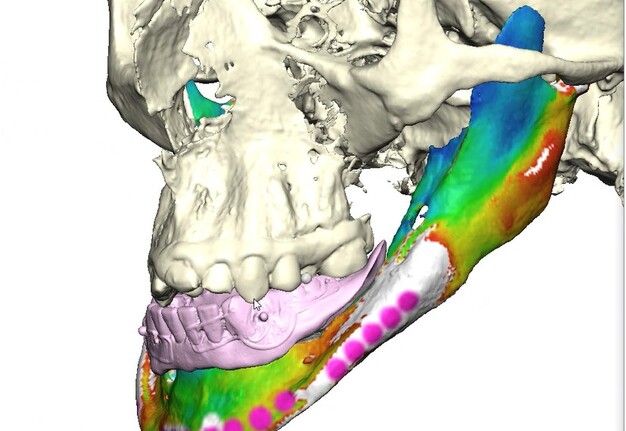
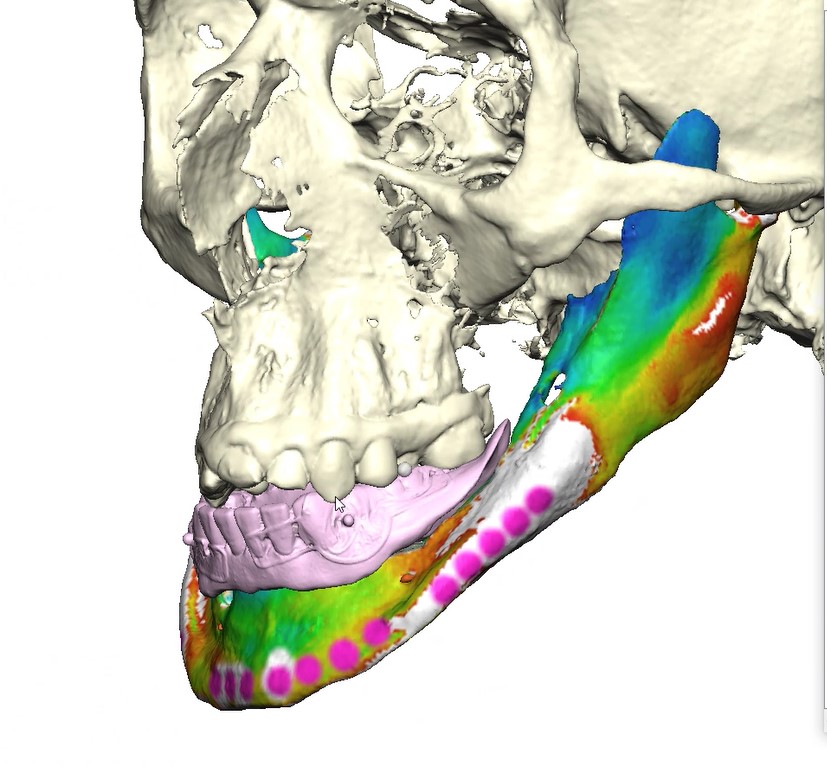
FIGURE 3. Virtual surgical planning (VSP) session with KLS Martin for the mandibular subperiosteal implant system with prototype, lateral view.
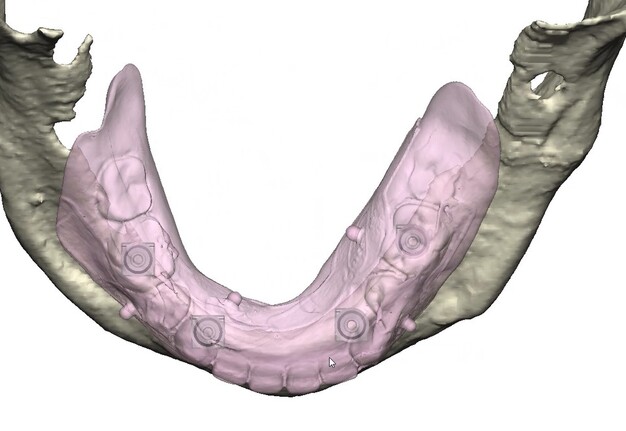
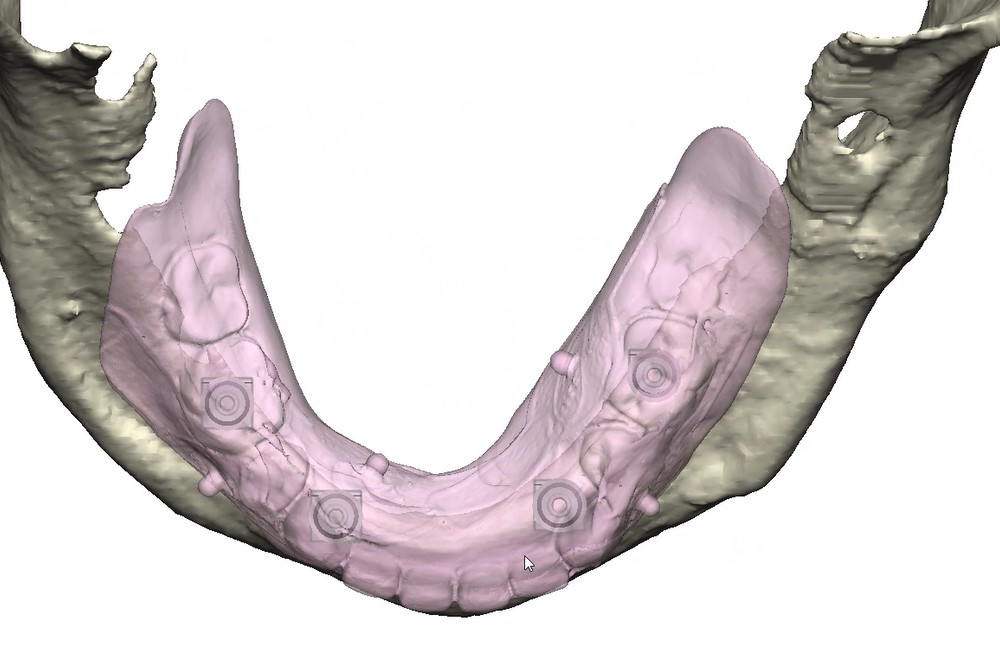
FIGURE 4. Virtual surgical planning (VSP) session with KLS Martin for the mandibular subperiosteal implant system with prototype, occlusal view.
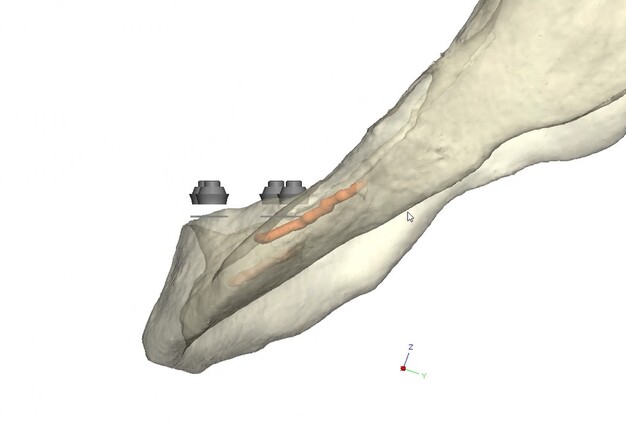
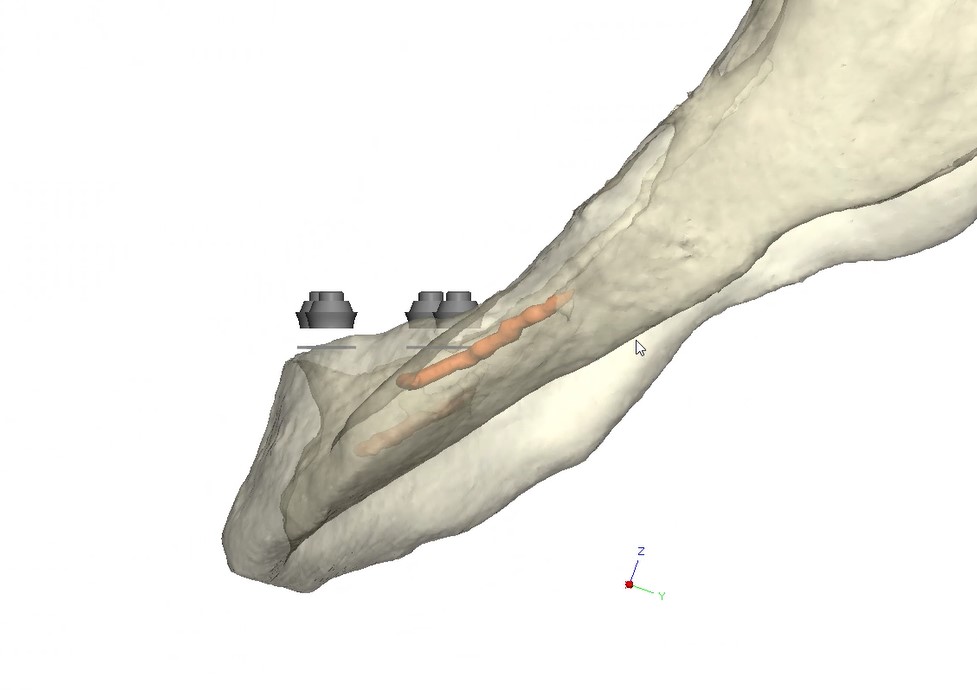
FIGURE 5. Side view showing the relative positioning of the multi-unit abutment in relation to the mandibular ridge.
A 3D-printed mandibular model with the subperiosteal system and prototype in place was also fabricated (Figs 6 and 7).


FIGURE 6. Printed 3D model of the mandible with the subperiosteal system in place and the mandibular prototype, frontal view.


FIGURE 7. Printed 3D model of the mandible with the subperiosteal system in place and the mandibular prototype, side view.
Under general anesthesia in an operating room setting, a crestal incision with bilateral releasing incisions was made on the mandible. Subperiosteal dissection extended to the inferior border of the mandible while preserving both mental nerves. A CAD-CAM bone reduction guide was rigidly fixated and used to perform alveoloplasty and predict fixation sites.
The custom titanium framework was trial seated and adapted accurately.
Due to the patient’s trismus, a transbuccal trocar system was used bilaterally to access posterior fixation sites, a technique commonly used in limited access mandibular fixation [17]. Locking screws were. placed under copious irrigation to achieve rigid stabilization (Fig 8).
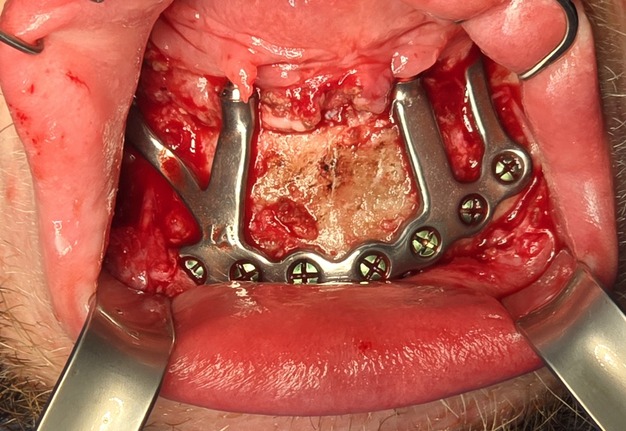
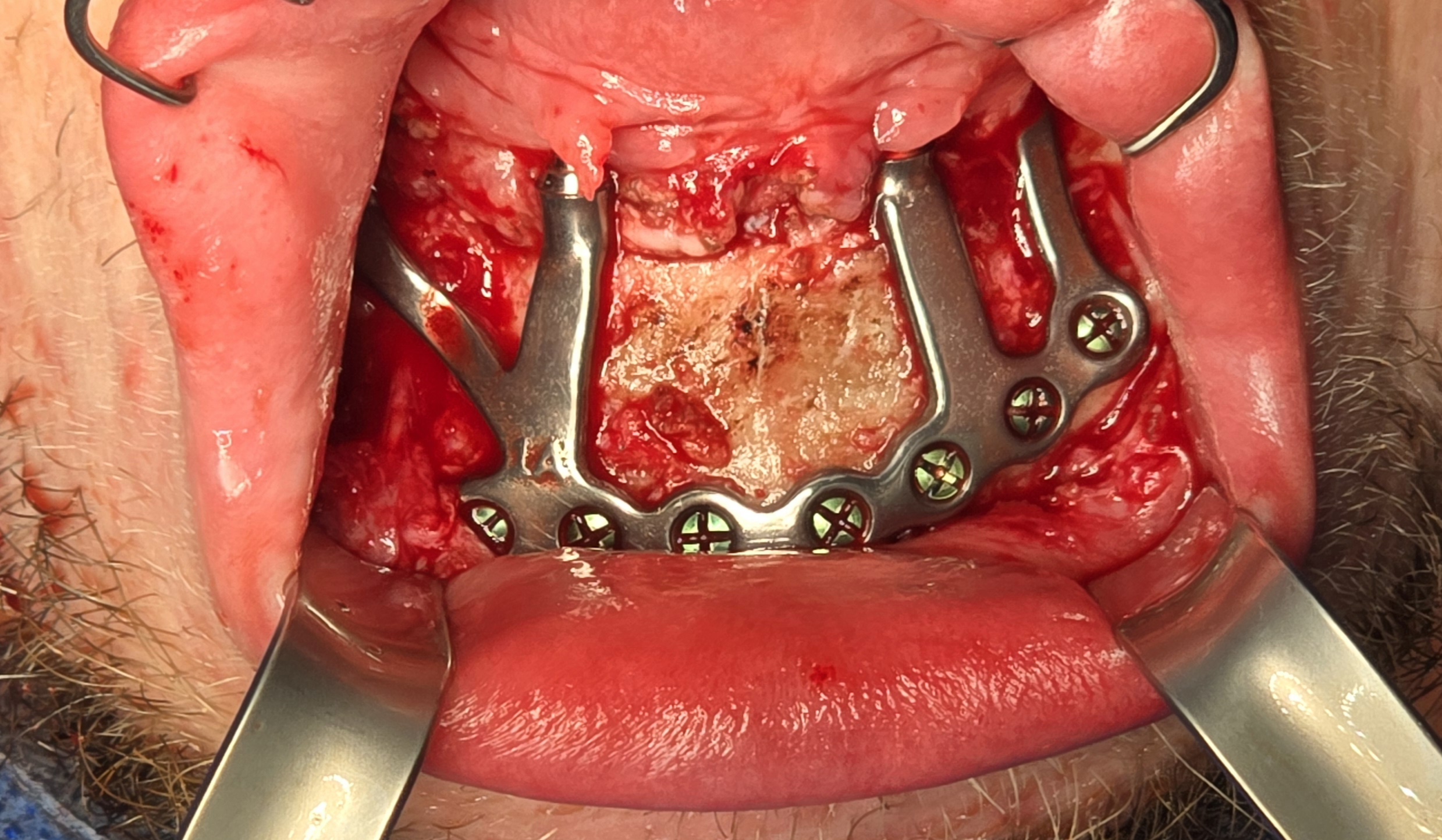
FIGURE 8. Intraoperative view demonstrating the seated subperiosteal implant fixed with multiple screws along the mandibular body.
A custom occlusal splint confirmed mount and prosthetic space. The site was closed with resorbable sutures intraorally and plain gut at trocar sites. Recovery was uneventful, and the patient progressed to prosthetic rehabilitation (Figs 9 and 10).


FIGURE 9. Intraoral view of the prototype in place with the patient in centric relation.


FIGURE 10. Limited oral opening, which precluded conventional impression and intraoral scanning techniques.
Digital-Analog Prosthetic Workflow
1. Prototype Removal
The existing prototype was removed using an extra-short multi-unit abutment (MUA) prosthetic screwdriver (BioHorizons). The patient shifted his mandible laterally to permit access to posterior screw channels (Fig 11).


FIGURE 11. Intraoral view without the prototype, showing multi-unit abutments emerging from the subperiosteal implant system.
2. Back-Pour Cast Fabrication
Analogs were attached to the prototype, and a back-pour cast was fabricated using Type IV Silky-Rock dental stone (Whip Mix). Reference notches were added to aid in digitization (Fig 12).

FIGURE 12. Back-pour cast fabricated from the provisional prototype with attached analogs and reference notches to facilitate accurate digitization of implant positions.
3. Digital Data Capture
-
Stereophotography scans of the cast were performed with the prototype in place and after removal with ICam4D scan bodies using Trios 4 Wireless Pod (3Shape) (Figs 12-14).
FIGURE 13. Back-pour cast without the prototype.
FIGURE 14. Extraoral photogrammetry using the ICam4D system with scan bodies in place, used to capture implant positions with an intraoral scanner (IOS).
-
ICam4D photogrammetry (Imetric 4D Imaging Sàrl) was used to captured implant positions with sub-5 µm trueness and sub-2 µm repeatability (Fig 15).
FIGURE 15. Extraoral photogrammetry using the ICam4D system with scan flags in place, used to capture implant positions with high trueness and repeatability.
4. Prototype Reseating and Records
Maxillary scanning was performed after prototype removal. Bite registration scans were captured after reseating the prototype and verifying occlusion. An updated prototype was fabricated, adjusted minimally, and worn for four weeks before fabrication of final prothesis.
5. Final Prosthesis
The refined prototype was rescanned on the back-pour cast, and a definitive monolithic implant supported fixed zirconia prosthesis was fabricated and successfully delivered (Figs 16 and 17).


FIGURE 16. Definitive mandibular full-arch monolithic zirconia prosthesis intraorally, demonstrating a high-water design for improved hygiene and cleanability.


FIGURE 17. Patient’s maximum opening with the definitive mandibular full-arch monolithic zirconia prosthesis in place.
DISCUSSION
This case required coordinated craniofacial reconstructive surgical planning with maxillofacial prosthodontic treatment. Despite early and repeat distraction, the patient demonstrated persistent mandibular hypoplasia and inadequate bone volume for traditional endosseous implants, consistent with long term outcomes reported in syndromic distraction osteogenesis patients who often show growth disturbances, relapse, and compromised bone biology [6-8, 15]. The failure of BMP-augmented grafting further reflects the unpredictable behavior of biologic augmentation in syndromic congenital mandibular deficiencies [16], supporting the indication for a CAD-CAM titanium subperiosteal implant.
Modern custom titanium subperiosteal frameworks have re-emerged as a viable treatment option in severe mandibular atrophy due to improved design precision, increased surface biocompatibility, and rigid multi-screw fixation [8, 9]. In this case, limited oral opening required a transbuccal approach for posterior fixation, which enabled secure access to the inferior border and is validated in mandibular fixation literature [17].
This case demonstrates how integrating ICam4D photogrammetry with cast digitization provides an effective alternative to conventional intraoral capture when access is restricted [12, 13]. Clinical studies confirm that photogrammetry systems yield highly accurate implant registration data, with trueness in the 17-30 µm range and clinically negligible precision errors [9-11]. Specialized systems such as ICam4D offer trueness under 5 um and repeatability under 2 µm [14], reinforcing clinical reliability.
Verification of passive seating, which could not be performed radiographically due to the inability to fit x-ray films intraorally, was carried out by visual confirmation on the fabricated physical cast followed by intraoral verification. The full arch implant supported fixed prosthesis was fully seated with no rocking or movement. A high-water design was utilized for enhanced hygiene, eliminating the need for tissue capturing and moulage. Passiveness was verified visually and tactically using a new sharp probe, with no evident gap. A one-screw test was performed to ensure there was no elevation on the opposite end. A screw resistance test was also performed, with all Vortex screws hand-tightened due to the inability to insert a torque wrench intraorally.
The prosthesis was fabricated from multilayered 3Y/5Y zirconia (Ivoclar Vivadent), directly milled without metal Ti-bases, and sealed with Teflon and resin composite. Occlusal contacts were checked, fine refinements were made, and the restoration was polished prior to final insertion.
Cast digitization has also been validated as a reliable substitute for intraoral scanning in restricted access cases. While minor distortions may occur, results remain clinically acceptable. This hybrid workflow, leveraging photogrammetry, cast digitization, and IOS of casts, allowed the successful fabrication of a well-fitting, functional, and esthetic zirconia prosthesis.
CONCLUSION
This case demonstrates how the integration of modern digital and surgical techniques can overcome the reconstructive and prosthetic limitations presented by cerebro-costo-mandibular syndrome (CCMS). In this patient, prior mandibular distractions and grafting procedures failed to achieve adequate bone volume for conventional endosseous implants. The use of a patient specific CAD-CAM titanium subperiosteal implant provided a precise and stable reconstructive foundation while avoiding the morbidity associated with vascularized bone grafting.
A combined digital-analog protocol using back-pour cast fabrication, IOS of casts, and ICam4D photogrammetry enabled the successful rehabilitation of a CCMS patient where traditional techniques were not viable. This reproducible workflow can serve as a valuable model for managing complex cases with severe intraoral access limitations. Together, these methods resulted in the successful rehabilitation of a syndromic, severely atrophic mandible with a passively fitting, functional, and esthetic full arch prosthesis.
This multidisciplinary protocol establishes a reproducible model for managing complex craniofacial cases where both surgical reconstruction and prosthetic restoration can be tailored to the specifics of an individual patient through precision digital technology.
Patient Consent
Written informed consent was obtained prior to the taking of pictures, videotapes or other electronic reproductions of medical or surgical condition or treatment, and the use of the pictures, videotapes or electronic reproductions, for treatment or internal or external activities consistent with the Hospital’s mission, such as education and research, conducted in accordance with Hospital policies.
Declaration of generative AI and AI-assisted technologies in the manuscript preparation process
During the preparation of this work, the authors used ChatGPT (OpenAI) to assist with language editing and formatting. After using this tool, the authors reviewed and edited the content independently and takes full responsibility for the content of the publication.
REFERENCES (17)
- Smith DW, Griffin JP, Spranger JW. The cerebro-costo-mandibular syndrome. J Pediatr. 1966;69(2):189-195.
- Donnai D, Barrow M, Winter RM. Cerebro-costo-mandibular syndrome: report of three cases and review. J Med Genet. 1987;24(9):573-579.
- Holder-Espinasse M, Abadie V, Cormier-Daire V, et al. Further delineation of cerebro- costo-mandibular syndrome: 20 new cases. Am J Med Genet A. 2004;128A(1):55-62.
- Kirschner RE, Low DW, Randall P, Bartlett SP, McDonald-McGinn DM, Zackai EH, et al. Airway management in neonates with craniofacial anomalies. Cleft Palate Craniofac J. 2003;40(3):221-226.
- McCarthy JG, Schreiber J, Karp N, et al. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992;89(1):1-8.
- Ow AT, Cheung LK. Meta-analysis of mandibular distraction osteogenesis: clinical applications and functional outcomes. Plast Reconstr Surg. 2008;121(2):54e-69e. https://doi.org/10.1097/01.prs.0000299285.97379.35.
- Peacock ZS, Sadove AM, Troulis MJ, Kaban LB. Long-term effects of distraction osteogenesis of the mandible: adverse dental outcomes and growth comparison with controls. J Oral Maxillofac Surg. 2018;76(3):607-615. https://doi.org/10.1016/j.joms.2017.12.034
- Gasparini G, Todaro M, De Angelis P, et al. Clinical outcomes of CAD-CAM subperiosteal implants for the rehabilitation of atrophic jaws. Dent J (Basel). 2024;12(8):241. https://doi.org/10.3390/dj12080241
- Abuduwaili K, Huang R, Song J, et al. Comparison of photogrammetric imaging, intraoral scanning and conventional impression accuracy of full-arch dental implant rehabilitation: an in vitro study. BMC Oral Health. 2025;25(1):753. https://doi.org/10.1186/s12903-025-06029-8
- Estibalez-Recasens M. Precision of stereophotogrammetry in complete arch implant positioning. J Prosthet Dent. 2025. https://doi.org/10.1016/j.prosdent.2025.01.005
- Revilla-León M, Gómez-Polo M, Gallucci GO, Özcan M. Accuracy of complete-arch implant scans by photogrammetry systems compared with intraoral scanners. J Prosthet Dent. 2025. https://doi.org/10.1016/j.prosdent.2025.02.009
- Emam NS, Öztürk C, Revilla-León M, Özcan M. Digitization accuracy and scannability of different prosthodontic materials. J Prosthet Dent. 2023;129(6):708-714. https://doi.org/10.1016/j.prosdent.2022.07.018
- Ellakany P, Revilla-León M, Özcan M. Accuracy of digital and 3D-printed casts vs conventional stone casts: a comparative study. J Prosthet Dent. 2020;124(5):632-639. https://doi.org/10.1016/j.prosdent.2019.10.023
- iMetric4D. New rules for fit: Full-arch lessons you didn't learn in dental school - what every implant dentist should know about microns, misfit, and modern tools. 2025. Accessed August 16, 2025. https://imetric4d.com/icam-photogrammetry-feature-comparison/
- Figueroa AA, Pruzansky S. Long-term results of mandibular distraction in craniofacial microsomia. Plast Reconstr Surg. 1999;104(3):458-467.
- Pogrel MA, Peled M. Mandibular reconstruction using BMP-2: long-term outcomes and complications. J Oral Maxillofac Surg. 2004;62(8 Suppl 2):34-40.
- Landes CA, Lipphardt R, Petruchin O, Schmelzeisen R. Transbuccal system for mandibular osteosynthesis: prospective clinical study. J Oral Maxillofac Surg. 2004;62(10):1177-1183.