
Mucous Plugs, Sialoliths, and Foreign Bodies of Salivary Glands: A Clinicosonographic Review
Manuscript received 11 March 2026
Revised 19 May 2026
Accepted 21 June 2026
Available online 30 June 2026
J Diagn Treat Oral Maxillofac Pathol 2026; 10: 100319.
DOI: https://doi.org/10.23999/j.dtomp.2026.6.100319
Under a Creative Commons license (CC BY-NC-SA 4.0)
HOW TO CITE THIS ARTICLE
Cherniak OS, Fesenko II, Demidov VH. Mucous plugs, sialoliths, and foreign bodies of salivary glands: A clinicosonographic review. J Diagn Treat Oral Maxillofac Pathol. 2026;10(6):100319.

INSTITUTIONAL REPOSITORY
https://ir.kmu.edu.ua/handle/123456789/1008
ABSTRACT
The goal of this narrative review is a comparative analysis of the ultrasound and macroscopic appearance of salivary gland mucous plugs with sialoliths and foreign bodies. The salivary sludge was also considered. In the world there are only two effective methods for diagnosing mucous plugs, ultrasonography and sialendoscopy. The first is simpler, cheaper and easier to perform, but more difficult to interpret for non-experienced clinicians, and the second is more difficult to perform, but easier to visualize and verify on the screen. While numerous cases of sialendoscopic images of mucous plugs in the parotid glands have been documented worldwide, sonographic images of mucous plugs in the Wharton’s duct have been noted by us in only one publication, and publications with sonograms of mucous plugs of the parotid glands, according to our literature search, are completely absent.
KEY WORDS
Ultrasonography, salivary glands, mucous plug, sialolith, foreign body, Wharton’s duct, Stensen’s duct
INTRODUCTION
Obstructive salivary gland disease (OSGD) is characterised by a history of recurrent pain and swelling of the gland [1]. Eating-induced pain (Farhadi et al., 2023) (synonym: salivary colics) and gustatory swelling (Yazbeck et al., 2023) are two most common symptoms of OSGD [2, 3]. OSGD is usually triggered by sialoliths, mucous plugs, foreign bodies, stricture, stenosis or a combination of them [4, 5]. Erkul and Gillespie (2016) describe stricture and stenosis as two types of salivary duct scar [6]. While sialoliths are well-studied both from the point of view of diagnostics [7-9] and management [10, 11], their clinical and sonographic comparison with mucous plugs [12] and foreign bodies [13] is still insufficiently elucidated. Therefore, the main goal of this article is a comparative analysis of the ultrasound and macroscopic appearance of salivary gland mucous plugs with sialoliths and foreign bodies. The salivary sludge was also considered.
MUCOUS PLUGS
Mucus plugs in other parts of the body are also a pathology in demand for research. For example, mucus plugs in the air passages [14]. There is a certain generally accepted difference in the spelling of the name of the plugs in thoracic surgery, pulmonology, and oral and maxillofacial surgery. Mucous plug of a major salivary gland is a soft, “buttery”, light pink/yellowish formation/obstruction in the duct caused by saliva stagnation or increased mucus concentration [15, 16]. Mucous plugs of salivary glands (Fig 1) are also known as mucus plugs, mucosal plugs, mucofibrinous plugs, fibrinous mucus plugs, fibromucinous plugs, or clots of fibrin [12, 17].
In 1935 Bruce Pearson described the passage of fibrinous plugs containing large number of eosinophils from the parotid ducts in children [18]. Unfortunately, macroscopic photographs of the plugs were not presented.
In 1978 the first report of the use of ultrasonography (USG) for salivary stone detection was published by Pickrell, Trought and Shearin in the Journal of Plastic Surgery [19]. US of a calculus in the parotid gland has been described in their case report paper.
The world’s first publication comparing the ultrasound and clinical (macroscopic) appearance of mucous plugs with salivary stone was published in May 2019 (treated in August 2014) [12]. Thus, 41 years have passed from the description of the USG picture of a sialolith to the description of the USG picture of a salivary gland mucous plug. Submandibular mucous plugs in the case of 2019 were sonographically detected and removed from the Wharton’s duct simultaneously with sialolith at the stages of treatment of exacerbation of salivary stone disease [12]. Clinically, submandibular mucous plug and sialolith (i.e., salivary stone) can be compared to “butter” and “stone” in terms of consistency to the touch [12].
Endoscopy historically emerged later than USG, so its use, in particular for the major salivary glands, only began in the early 1990s (Nahlieli, 2004) [20]. In 1991, Konigsberger et al., highlighted endoscopic controlled laser lithotripsy in the treatment of sialolithiasis [21]. In 1990, 1991, and 1993, Katz described endoscopy of the major salivary glands and demonstrated how it is possible to extract sialoliths via the natural passages using a miniaturized basket catheter, avoiding the need for more extensive surgery [22-24].
In 1997 (Nahlieli et al.), there were no mentions of endoscopic images of mucous plugs, but mainly images of sialoliths and statistical data on endoscopic results [25].
Marchal et al. (1999) upon their description of interventional sialendoscopy also demonstrate endoscopic images exclusively of sialoliths [26].
In 2002, Marchal et al., in their report of submandibular diagnostic and interventional sialendoscopy, demonstrate approaches to endoscopic removal of culculi [27]. We confirm the Marchal’s data (2005), sialendoscopy is incredibly excellent for visualizing the ductal system of the salivary glands with their ramifications [28]. We were unable to determine exactly in which year the endoscopic image of mucous plugs of salivary was first published. The earliest such image was found in the book chapter by Marchal in 2007 [29]: “Floating mucous plugs can be seen alone or in conjunction with salivary stones or stenotic processes. It has been suggested that these “mucous plugs” present in the ductal system may represent the nidus for the development of calculi”. That is, 17 years have passed since the application of endoscopy for the management of sialolithiasis. Yu et al. (2008) presented sialendoscopy images of parotid mucous plug upon treatment of chronic obstructive parotitis [30].
As of 2026, the appearance of mucous plugs through sialendoscopy has been described in a much larger number of studies. In 2021, Fusconi et al. devoted the highly important article to interpretation of the mucous plugs through sialendoscopy [16]. In their study, the mucous plugs were pale pink. The chronology of the introduction of sialendoscopy is detailed in Fritsch’s work (2009) [31].
Chikamatsu et al. (2006) presented two sialodochitis fibrinosa patients with recurring bilateral parotid swelling [32]. In both patients, secretion of mucous plugs containing numerous eosinophils was observed from Stensen’s ducts. The article’s black and white photo shows a 2-cm mucous plug extruded from the main parotid duct. Our literature search did not yield data on the ultrasound appearance of mucous plugs of the parotid or sublingual glands. Thus, the 2019 publication, at the time of writing, was the first clinical and ultrasound presentation of mucous plugs of the main duct of the submandibular gland [12].
Karwowska and Turner (2021) [5] state the following: “The submandibular glands have a higher concentration of mucous cells than the parotid glands, and are thus more likely to form obstructive mucous plugs. When a mucous plug is the sole cause of obstruction, it is referred to as a primary mucous obstruction. If a mucous plug occurs in conjunction with another obstructive process, such as a sialolith or a stricture, it is referred to as a secondary mucous obstruction.” Although some authors believe that the formation of mucous plugs is more likely in the submandibular glands, other sources indicate a higher probability of detecting plugs in the parotid glands. According to Sánchez Barrueco, Díaz Tapia, et al. (2025) in 84% of cases, mucous plugs occur in the parotid glands [4]. In 16% of cases, mucous plugs occur in the submandibular glands [4].
Floating mucous plugs can be seen alone or in conjunction with sialoliths or stenotic processes (Marchal, 2007) [27]. It has been suggested that these “mucous plugs” present in the ductal system may represent the nidus for the development of calculi (Marchal, 2007) [27]. The author demonstrate unique sialoendoscopic images, namely: (1) Mucous plug attached to the calculus which impairs intraductal vision, (2) mucosal plug which is mechanically detached by gently tapping on the calculus with the laser fiber tip, and (3) extraction of this plug using a wire basket [27].
According to sialoendoscopy, with swelling of the submandibular glands, mucous plugs are found in 3% of cases, stones in 91% of cases, and stenosis in 6% of cases (Chuangqi Yu et al., 2013) [33]. With swelling of the parotid glands, completely different data are noted: mucous plugs are found in 14% of cases, sialoliths in 11% of cases, and stenosis in 75% of cases.
Gür et al. in 2023 highlighted yellowish fibromucinous plugs of the parotid glands upon Kussmaul disease (also known as sialodochitis fibrinosa) [34, 35]. Tymofieiev (2025) describes the saliva obtained with such parotid sialadenitis as stagnant and viscous saliva with strands (flakes) of fibrin [36].
Baer et al. (2017) in their study about eosinophilic sialodochitis highlighted redefinition of “allergic parotitis” and “sialodochitis fibrinosa” [17]. The authors did a good review of the literature on mucous plugs in this type of parotitis [17]. Here is their data: “The mucus plugs measured up to 3 cm in length (Pearson, 1935; Yoshioka et al., 1997) [18, 37] with variable consistency: sometimes gelatinous (Pollak et al., 2009; Shimada et al., 2006; Tsuchiya et al., 2012) [38-40], but sometimes firm enough to form casts of the ducts (Motosugi et al., 1998) [41]”.
Hayashi et al. (2016) presented gelatinous plug (clots of fibrin) discharged from parotid papilla [42]. Pressure on parotid glands bilaterally induced discharge of gelatinous plugs from parotid papillae. No discharge of pus and no calcifications were observed.
Salazar and Celestin (2020) reported about microscopic features of mucofibrinous plugs of the submandibular glands upon Kussmaul disease [43].
Baer et al. (2017) presented unique mucus plug cytology data [17]. Mucus plug expressed from Wharton’s duct with gland massage showed numerous eosinophils. Chuangqi et al. (2013) described how 4 polyps and 7 mucus plug cases were treated successfully by forceps and continuous rinsing under sialoendoscopy [33].
The shape of the mucous plugs on sialoendoscopic images of the parotid gland ducts (Jung et al., 2025) was elongated, unlike mucous plugs of the submandibular gland duct (Cherniak and Fesenko, 2019) study [44, 12]. Mucous plugs of the submandibular glands have isoechoic heterogeneous ultrasound appearance and no acoustic shadowing [12].
Pang et al. (2023) described a rare case of sialendoscopic removal of metastatic adenocarcinoma in a mucous plug from Stensen’s duct [45].
According to Steck et al. (2016), most of endoscopies (85%) were performed under general anesthesia in an outpatient fashion, but the procedure can be performed under local anesthesia too [46].
It is interesting that surgeon-performed ultrasound for chronic obstructive sialadenitis helps predict sialendoscopic findings and outcomes (Larson et al., 2017) [6].
The identified mucous plugs only in the ducts of the parotid and submandibular glands emphasize that the anatomy of these ducts and the physiology of these glands are favorable for the formation of these intraductal formations.
SIALOLITHS
While the presence of mucous plugs has been reliably established endoscopically, by USG, macro- and microscopically in the parotid and submandibular glands and their ducts, sialoliths have been detected in all major salivary glands [8, 47-50] as well as in the minor ones [51-53].
Zenk et al. (2012) and Sánchez Barrueco, López-Acevedo Cornejo, et al. (2025) detailed theories about formation of sialoliths [54, 15]. Three possible substrates for the formation of the initial core [15]: (1) floating mucoid materials in the Wharton duct (generically referred to as a mucus plug) [12], (2) vesicles filled with organic matter or lipid droplets [55] that give rise to so-called sialomicroliths, and (3) a foreign body that penetrates retrogradely from the oral cavity [13].
In 75.68% of cases, sialoliths occur in the submandibular glands and its ducts (Figs 2 and 3) (Sánchez Barrueco, Díaz Tapia, et al., 2025) [4]. In 24.32% of cases, sialoliths occur in the parotid glands and its ducts (Figs 4 and 5) [4]. The incidence of sublingual sialoliths has been reported as 0 to 6.4% (Hong and Yang, 2003) [58]. Interestingly, numerous sialoliths can be found in the sublingual gland, which resemble phleboliths in shape, namely pearl-shaped [59, 60].
Endoscopic classification of salivary lithiasis is perfectly described by Marchal et al. (2008) [61]. An interesting element of this classification is the division into floating and fixed [61]. It has already been proven that sialolith flotation can be verified using USG (Tymofieiev and Cherniak, 2019) [62].
Lustmann et al. (1990) found swelling to be present in 94% of their 245 cases of sialolithiasis, with pain occurring in 65.2%, the presence of purulence in 15.5%, and complete lack of symptoms in 2.4% of their cases [63, 64].
Our team, considering such diagnostic options as sialendoscopy, sialography, radiography, computed tomography and USG, considers the latter method to be the easiest, simplest and safest way to verify salivary calculi. How reliable is USG in the assessment of sialolithiasis is described in the article by Terraz et al. (2013) [65]. A proposal for standardized USG analysis of the salivary glands is described in detail by Hoffman et al. (2024) [66]. Typically, sialoliths are visualized as hyperechoic curved lines with posterior acoustic shadowing.
Howlett et al. (2004) have provided an excellent sonographic description and images of the submandibular gland and its appearance in sialolithiasis [67].
Bimanual palpation (i.e., two-handed palpitation) during USG (digital palpation of the floor of mouth with one hand while externally applying the probe with the other hand) can facilitate visualization of ductal stones (Orloff et al., 2009) [68]. The bilateral glands should always be examined for comparison and identification of individual differences, unilateral diseases, and systemic processes [68].
With USG, the difficulty of establishing the exact localization of a sialolith, mucous plug, or foreign body is higher in areas of the accessory parotid gland and due to the significant arborization in parotid gland itself (Amiel et al., 2024) [57]. The computed tomography sialography is recommended in such cases [57]. Despite intra- and periparenchymal calculi are rare (Bodner, 1999) [48] we present a 57-year-old male with a sialolith located between the capsule and the gland parenchyma (Fig 5B). Oliveira et al. (2014) highloghted a bedside emergency ultrasound in a case of acute parotid duct sialolithiasis [9]. Numerous studies have analyzed the use of ultrasound in sialolithiasis, and each of them is worth considering [69-78].
Hosokawa et al. (2023) emphasized that USG is often the first modality of choice for pediatric patients with OSGD due to the absence of radiation exposure and sedation during radiological examination [73]. Compared with adult calculi, paediatric calculi tend to be located on the distal side of the duct (i.e., closer to the sublingual papilla) (Hosokawa et al., 2023; Chung et al., 2007) [73, 79].
Kim et al. (2013) summarized the clinical data of young children with parotid sialolithiasis [80]. Cases of patients aged 2 to 5 years were analyzed [80]. In all cases, sialoliths were in the Stensen’s duct [80].
Speaking about radiological examinations, it is worth noting that classic laminated appearance is the characteristic appearance of salivary stones on radiographs, as confirmed in Figure 2A (Benson, 2014) [81].
Kraaij et al. (2014) described salivary microlith (i.e., sialomicrolith) [82] and Mostafavi Tabatabaee et al. (2019) provided a literature review of giant salivary sialoliths larger than 30 mm (i.e., salivary megaliths) [83]. When detecting rounded calcifications in the salivary gland area, it is important to conduct differential diagnosis with arteriovenous malformations [84]. The submandibular gland was previously named as submaxillary gland. Therefore, inflammation of this gland (i.e., sialadenitis) was called submaxillitis. Some surgeons continue to use this term today. Teymoortash et al. (2003) proved through serial histological examination of the entire Wharton’s duct in four samples revealed no anatomical correlation for the presence of a sphincter [85].
Kopeć et al. (2013) presented an algorithm of salivary gland obstructive pathology treatment, according to Koch et al. (2009) [11, 10]. The classic surgical approach for submandibular gland removal is open, transcervical approach (Beahm et al., 2009) [86]. Submandibular gland surgery using this approach is described in an excellent step-by-step manner with images in the publication by Tymofieiev (2007) [87].
Savchuk and Fesenko in 2021 demonstrated a transcutaneous removal of sialolith with a flow of pus in a patient with phlegmon of the flour of mouth and lateral neck due to the exacerbation of the chronic calculous submaxillitis [88].
There are important publications about sialolithiasis in an accessory submandibular gland and residual Wharton’s duct after excision of a submandibular gland [89, 90]. Therefore, it is worth understanding this anatomical feature of the gland.
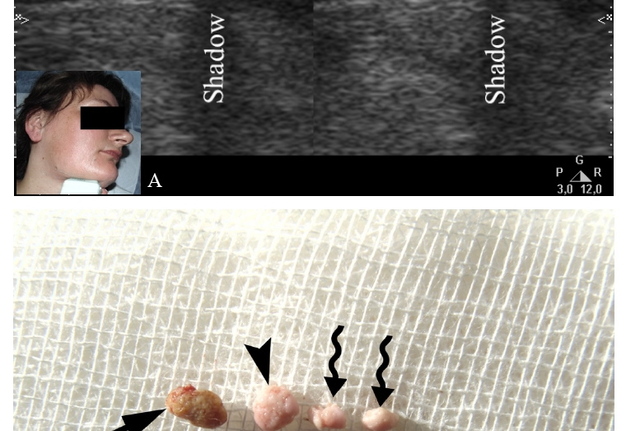
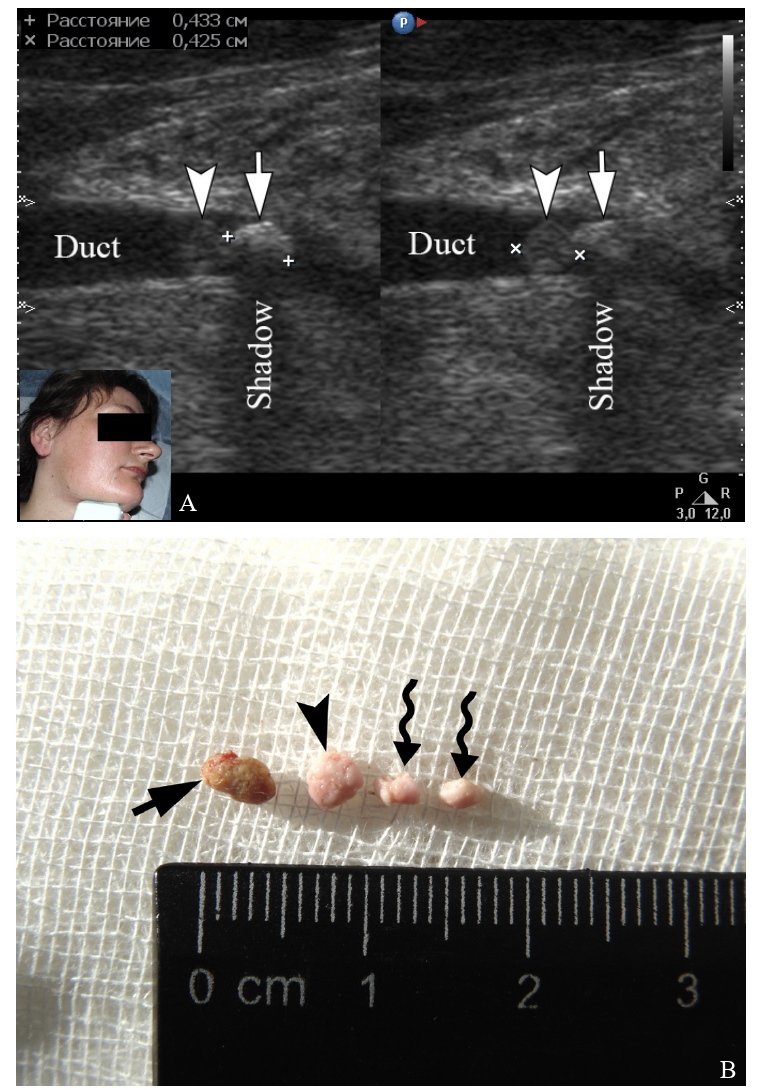
FIGURE 1. A 30-year-old female with exacerbation of chronic obstructive sialadenitis of the right submandibular gland as of August 19, 2014. Gray-scale ultrasound (A) shows a sialolith (indicated by “+” calipers) in the middle third of the dilated Wharton’s duct (Duct), secondary mucous obstruction (indicated by “×” calipers), and collected suppurated saliva. Mucous plug visualized as isoechoic heterogenous round shape body with no acoustic shadowing. (B) Sialolith (arrow), mucous plug (arrowhead) visualized on sonogram, and two other mucous plugs (waved arrows) after removal. The size of the removed mucous plug fully corresponds to its size on ultrasound.
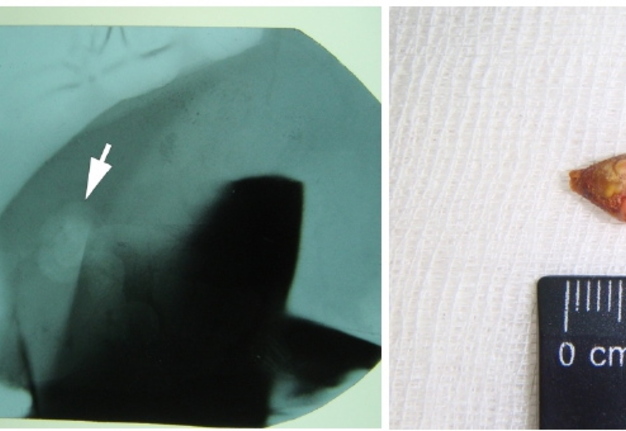
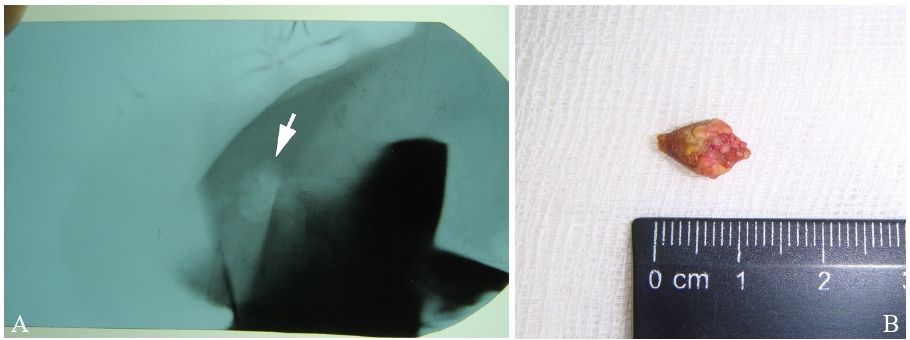
FIGURE 2. Mandibular occlusal radiograph (A) shows a classic clearly laminated structure of sialolith (arrow) located in distal portion of the Wharton’s duct of the submandibular gland as of October 16, 2015. (B) The removed calculus has a granular surface and a teardrop shape with a total length of more than 1.0 cm.
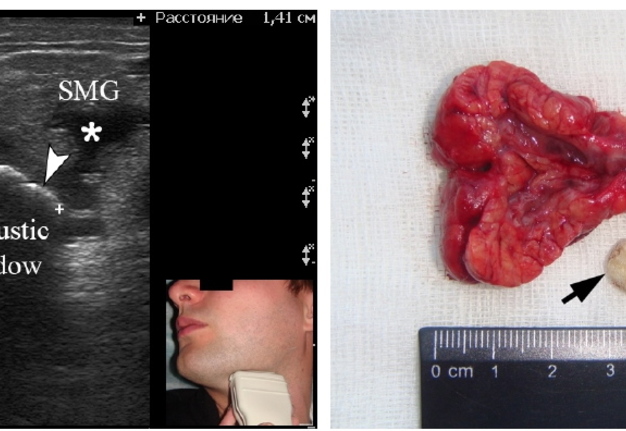
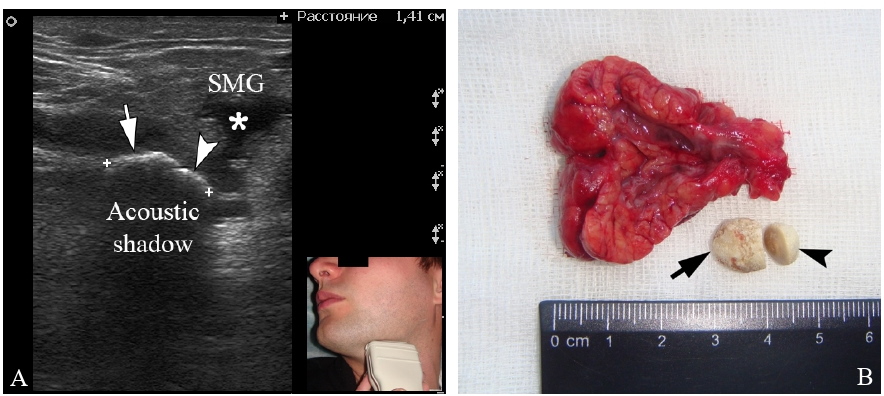
FIGURE 3. A 29-year-old male with sialolithiasis of the submandibular gland (SMG) with larger (arrow) and smaller (arrowhead) sialolith located in the hilum of November 04, 2014. (A) Gray scale ultrasound: Asterisk labels dilated intraglandular duct. (B) Gland and sialoliths after removal (arrow corresponds to a larger stone on ultrasound, and the arrowhead corresponds to a smaller one). Clinical image demonstrates position of the probe.
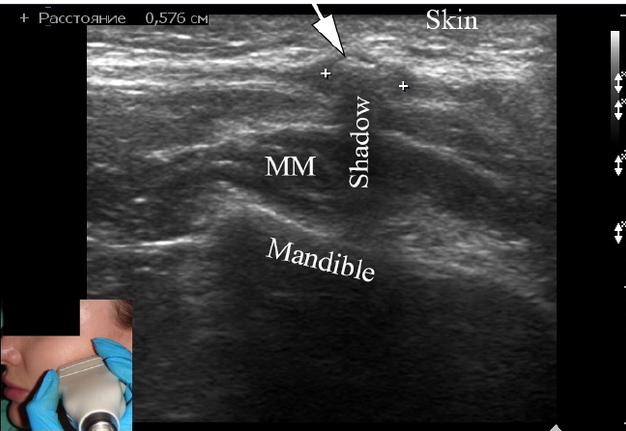
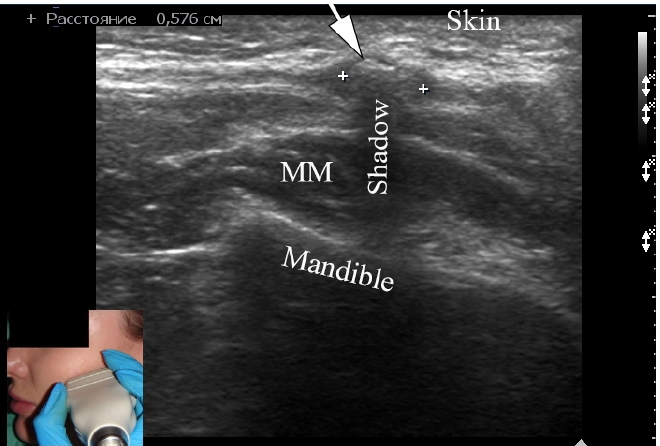
FIGURE 4. A 32-year-old female with calculus (arrow) of the parotid gland as of June 13, 2024. Gray scale ultrasound shows hyper-echoic reflex (labeled by “+” calipers) with posterior acoustic shadow (Shadow) caused by 0.57-cm long calculi. The stone was easily bimanually palpated. MM, masseter muscle. Probe was located close to a line connecting the tragus and the mouth corner (Iwanaga et al., 2026) [56]. The patient periodically notes swelling in the parotid area on the left when eating and bursting pain. The stone lies at a depth of 2.9 mm from the skin surface. In such cases, it is sometimes difficult to pinpoint the exact location of the sialolith without computed tomography sialography due to the presence of the accessory parotid gland and ductal arborization (Amiel et al., 2024) [57].
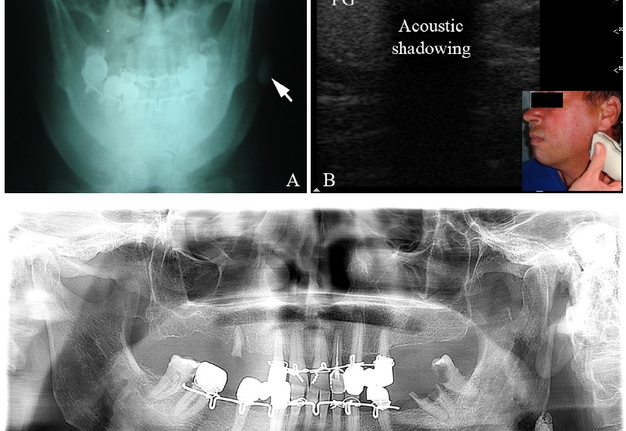
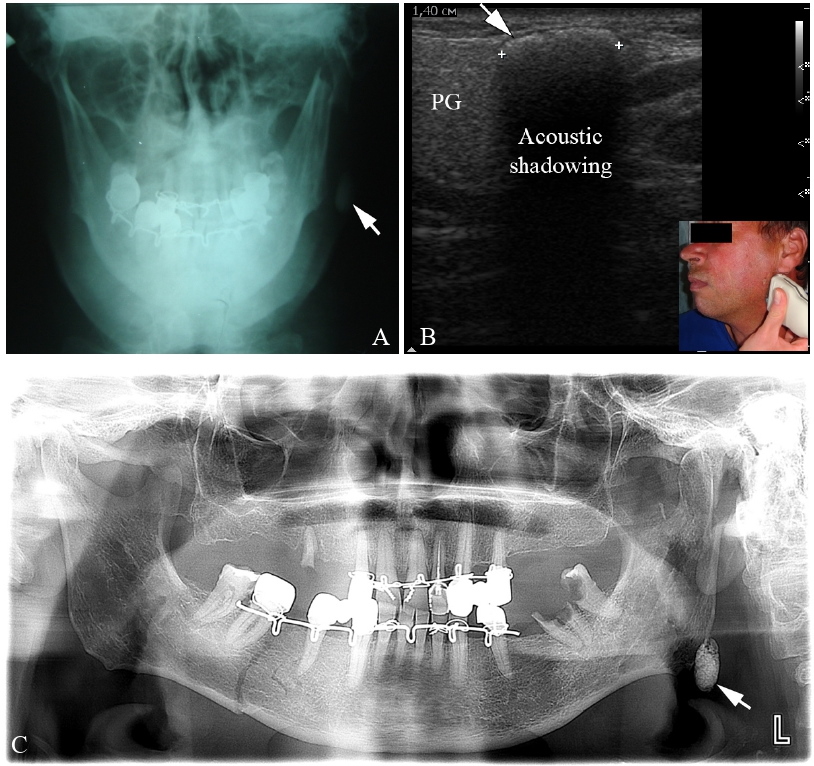
FIGURE 5. A 57-year-old male with sialolith (arrow) of the left parotid gland as of May 16, 2015. The calculus was discovered accidentally during the treatment of a bilateral mandibular fracture. The patient had no history of complaints of salivary colic. (A) Antero-posterior radiography of the jaws; (B) Gray scale ultrasound of the parotid gland shows hyper-echoic reflex (labeled by “+” calipers) with acoustic shadowing caused by a 1.4-cm long salivary stone near the lower pole of the parotid gland; (C) panoramic radiograph. Ultrasound indicates the location of the stone under the parotid fascia (i.e., parotid capsule). Clinical image demonstrates position of the probe. The stone was very easily palpated through the skin.
FOREIGN BODIES
Fish bone, fingernail, vegetal nidus, thorn, piece of hair, metal body, and other particles are among numerous foreign bodies penetrated the major salivary glands [13]. Savchuk and Nozhenko (2020) performed and interesting report of a foreign body retrograde migration to the intraglandular duct of the submandibular gland with a developing of foreign body-induced sialolithiasis [13]. Additionally, an analysis of USG, surgery, and literature published during the last 124 years was conducted.
Foreign bodies can enter the parotid gland both intraoral through the Stensen’s duct and extraoral through penetration of a foreign body through a wound on the skin Ahmed et al. (2015) [91].
Gill et al. (2016) described in their study an ultrasound appearance of foreign body (fish bone) in the parotid gland [92]. Paper included gray scale sonogram and cine loops.
In 2025, Zheng et al. published a case with Stensen’s duct penetration and sialolith formation as a rare complication of thread lifting surgery [93]. Sialendoscopy revealed calculus deposited on a “thread-like foreign body”.
Luo et al. (2022) illustrated transcutaneous and transoral USG precisely located the splinter within Wharton’s duct [94]. Shortly thereafter, the bamboo splinter was spontaneously discharged while eating, which allowed complete remission of pain and swelling.
Oz et al. (2022) presented an ultrasound image of a foreign body with vegetative morphology, which settles into the parotid gland by retrograde migration [95].
Also, numerous fish bone-induced sialoliths are dscribed in details [13, 96, 97].
Interestingly, Smith and Jones (2024) demonstrated the possibility of the foreign body ultrasound verification in dogs in the article “Ultrasound diagnosis and sialadenectomy confirming a mandibular salivary gland vegetative foreign body and chronic sialadenitis in a dog” [98].
Removal of a foreign body depends on localization [13], in principle, almost the same as removal of a stone.
SLUDGE
Salivary sludge is thick saliva with high protein content that can block salivary duct [99]. Ductal sludge (i.e., salivary sludge) sonographic visualization is featured in a book chapter by Bradley (2000) [100]. According to Hoffman and Iowa Head and Neck Protocols (2017), the dynamic movement of sludge is primarily observed via dynamic real-time ultrasound imaging (sonopalpation) [69].
The term “sludge” is also used in general medicine, for example “biliary sludge” (Lee et al., 2018) [102]. Sludge is a collection of the precipitants of bile that collects in layers within the gallbladder and appears sonographically as mildly echogenic material without acoustic shadowing [101].
CONCLUSION
In the world there are only two effective methods for diagnosing mucous plugs, ultrasonography and sialendoscopy. The first is simpler, cheaper and easier to perform, but more difficult to interpret for non-experienced clinicians, and the second is more difficult to perform, but easier to visualize and verify on the screen.
Summing up the comparison of such pathological objects of the salivary glands as mucous plugs, sialoliths, foreign bodies and salivary sludge, it is worth noting the extremely high diagnostic capabilities of USG.
Table 1 demonstrates the sonographic and clinical comparison of pathological objects of the salivary glands [102].
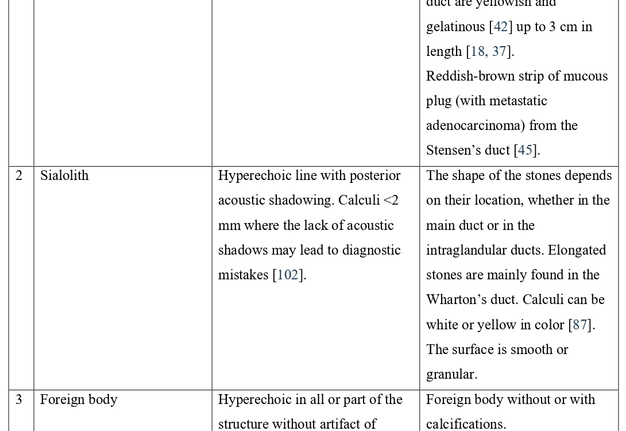
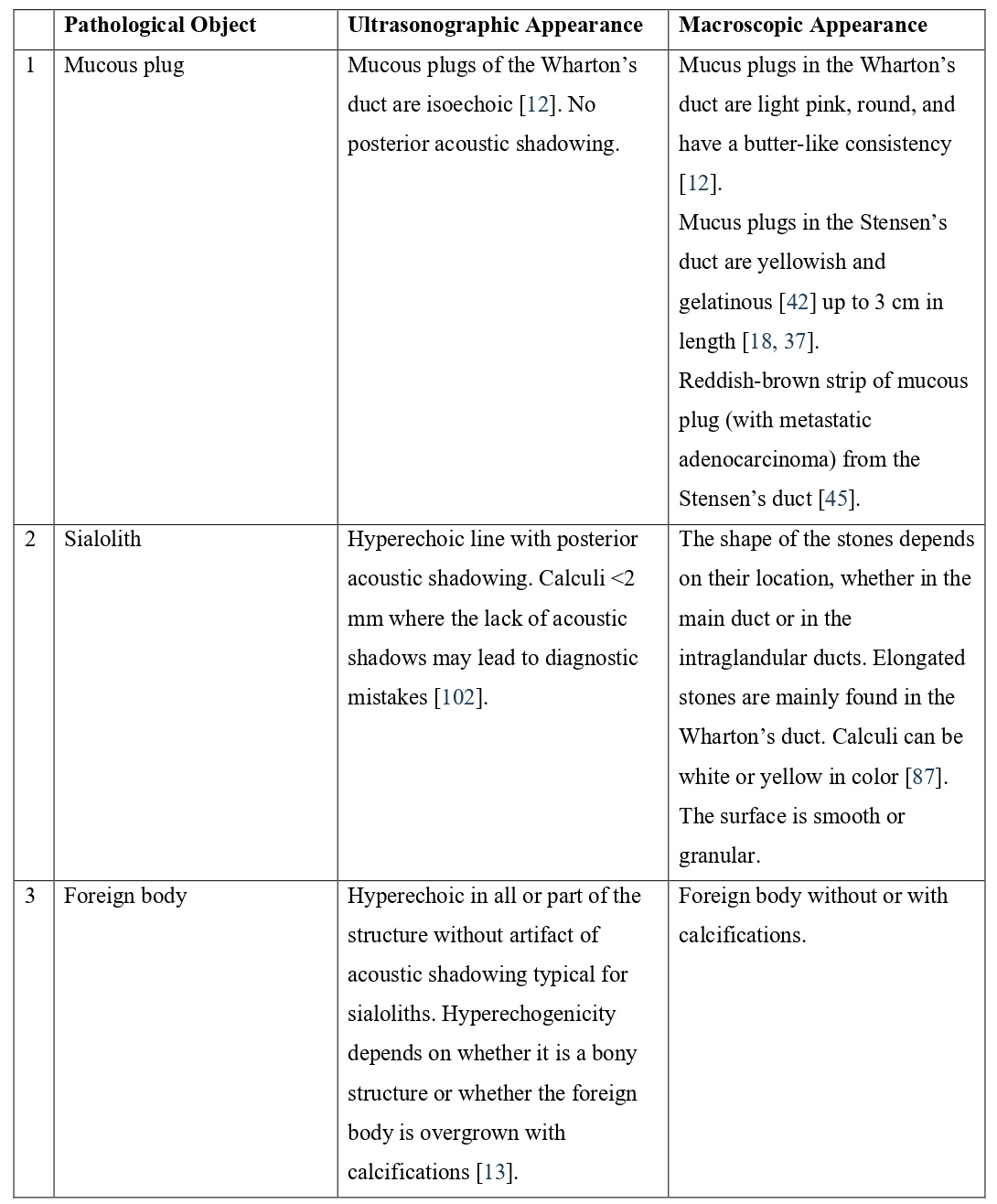
TABLE 1. Pathological Objects of the Salivary Glands: Ultrasonographic and Clinical Comparison.
DISCLOSURES
Author Contributions: Concept and Design – I.I.F.; Literature Search – O.S.C.; Writing – I.I.F., O.S.C.; Critical Review – V.H.D.
Declaration of Interests: The authors have no conflicts of interest to declare.
Informed Consent: Written consent was obtained from patients for publication of photographs.
Fundings: No funding was received for this study.
Peer-Review: Externally peer-reviewed.
AI Statement: The authors declared that artificial intelligence was not used in this article.
REFERENCES (102)
-
Atienza G, López-Cedrún JL. Management of obstructive salivary disorders by sialendoscopy: a systematic review. Br J Oral Maxillofac Surg. 2015;53(6):507-519. https://doi.org/10.1016/j.bjoms.2015.02.024
-
Farhadi M, Mohebbi S, Daneshi A, et al. The therapeutic outcome of sialendoscopy in patients with sialoadenitis. Iran J Otorhinolaryngol. 2023;35(127):91-96. https://doi.org/10.22038/ijorl.2023.63433.3174
-
Yazbeck A, Iwanaga J, Walocha JA, et al. The clinical anatomy of the accessory submandibular gland: a comprehensive review. Anat Cell Biol. 2023;56(1):9-15. https://doi.org/10.5115/acb.22.118
-
Sánchez Barrueco A, Díaz Tapia G, Alcalá Rueda I, et al. Quantifying the impact of chronic obstructive sialadenitis on quality of life. J Clin Med. 2025;14(21):7560. https://doi.org/10.3390/jcm14217560
-
Karwowska NN, Turner MD. Etiology, diagnosis, and surgical management of obstructive salivary gland disease. Front Oral Maxillofac Med. 2021;3:17. https://doi.org/10.21037/fomm-20-73
-
Larson AR, Aubin-Pouliot A, Delanges E, et al. Surgeon-performed ultrasound for chronic obstructive sialadenitis helps predict sialendoscopic findings and outcomes. Otolaryngol Head Neck Surg. 2017;157(6):973-980. https://doi.org/10.1177/0194599817728867
-
Gonçalves M, Schapher M, Iro H, et al. Value of sonography in the diagnosis of sialolithiasis: comparison with the reference standard of direct stone identification. J Ultrasound Med. 2017;36(11):2227-2235. https://doi.org/10.1002/jum.14255
-
Demidov VH, Khrulenko SI. Sialoliths of submandibular gland and Wharton’s duct: orthopantomography. J Diagn Treat Oral Maxillofac Pathol. 2021;5(7):77-86. https://doi.org/10.23999/j.dtomp.2021.7.1
-
Oliveira LG, Hurst ND, Magajna PW. Bedside emergency ultrasound in a case of acute parotid duct sialolithiasis. J Emerg Med. 2014;47(2):e49-e51. doi:10.1016/j.jemermed.2014.04.022
-
Koch M, Zenk J, Iro H. Algorithms for treatment of salivary gland obstruction. Otolaryngol Clin N Am. 2009;42(6):1173-1192. https://doi.org/10.1016/j.otc.2009.08.002
-
Kopeć T, Wierzbicka M, Szyfter W, Leszczyńska M. Algorithm changes in treatment of submandibular gland sialolithiasis. Eur Arch Otorhinolaryngol. 2013;270(7):2089-2093. https://doi.org/10.1007/s00405-013-2463-7
-
Cherniak OS, Fesenko II. Effectiveness of ultrasound in verification of the mucus plugs and sialoliths of the Wharton`s duct. J Diagn Treat Oral Maxillofac Pathol. 2019;3(5):144-153. https://doi.org/10.23999/j.dtomp.2019.5.3
-
Savchuk LA, Nozhenko OA. Foreign body retrograde migration to the intraglandular duct of the submandibular gland with a developing of foreign body-induced sialolithiasis: analysis of ultrasonography, surgery, and literature published during last 124 years. J Diagn Treat Oral Maxillofac Pathol. 2020;4(3):53-59. https://doi.org/10.23999/j.dtomp.2020.3.2
-
Panchabhai TS, Mukhopadhyay S, Sehgal S, et al. Plugs of the air passages: A clinicopathologic review. Chest. 2016;150(5):1141-1157. https://doi.org/10.1016/j.chest.2016.07.003
-
Sánchez Barrueco Á, López-Acevedo Cornejo MV, Aragonés Sanzen-Baker W, et al. Evolutionary conformation model of salivary gland lithiasis. Front Oral Health. 2025;6:1610977. https://doi.org/10.3389/froh.2025.1610977
-
Fusconi M, Meliante PG, Pagliuca G, et al. Interpretation of the mucous plug through sialendoscopy. Oral Dis. 2022;28(2):384-389. https://doi.org/10.1111/odi.13796
-
Baer AN, Okuhama A, Eisele DW, et al. Eosinophilic sialodochitis: redefinition of 'allergic parotitis' and 'sialodochitis fibrinosa'. Oral Dis. 2017;23(7):840-848. https://doi.org/10.1111/odi.12595
-
Bruce Pearson RS. Recurrent swelling of the parotid glands. Arch Dis Child. 1935;10(59):363-376. https://doi.org/10.1136/adc.10.59.363
-
Pickrell KL, Trought WS, Shearin JC. The use of ultrasound to localize calculi within the parotid gland. Ann Plast Surg. 1978;1(6):542-546. https://doi.org/10.1097/00000637-197811000-00003
-
Nahlieli O. Salivary gland inflammatory disorders in children. In: Kaban LB, Troulis MJ, eds. Pediatric Oral and Maxillofacial Surgery. Elsevier Science; 2004:ch 13. https://doi.org/10.1016/B978-0-7216-9691-1.50018-1
-
Königsberger R, Feyh J, Goetz A, et al. Die endoskopisch kontrollierte Laserlithotripsie zur Behandlung der Sialolithiasis [Endoscopic controlled laser lithotripsy in the treatment of sialolithiasis]. Laryngorhinootologie. 1990;69(6):322-323. https://doi.org/10.1055/s-2007-998200
-
Katz P. Un nouveau mode d'exploration des glandes salivaires: la fibroscopie [New method of examination of the salivary glands: the fiberscope]. Inf Dent. 1990;72(10):785-786.
-
Katz P. Endoscopie des glandes salivaires [Endoscopy of the salivary glands]. Ann Radiol (Paris). 1991;34(1-2):110-113.
-
Katz P. Nouvelle thérapeutique des lithiases salivaires [New treatment method for salivary lithiasis]. Rev Laryngol Otol Rhinol (Bord). 1993;114(5):379-382.
-
Nahlieli O, Baruchin AM. Sialoendoscopy: three years' experience as a diagnostic and treatment modality. J Oral Maxillofac Surg. 1997;55(9):912-920. https://doi.org/10.1016/s0278-2391(97)90056-2
-
Marchal F, Dulguerov P, Lehmann W. Interventional sialendoscopy. N Engl J Med. 1999;341(16):1242-1243. https://doi.org/10.1056/NEJM199910143411620
-
Marchal F, Barki G, Dulguerov P, et al. Submandibular diagnostic and interventional sialendoscopy: new procedure for ductal disorders. Ann Otol Rhinol Laryngol. 2002;111(1):27-35. https://doi.org/10.1177/000348940211100105
-
Marchal F. Endoscopie des canaux salivaires: toujours plus petit, toujours plus loin? [Salivary gland endoscopy: new limits?]. Rev Stomatol Chir Maxillofac. 2005;106(4):244-249. https://doi.org/10.1016/s0035-1768(05)85853-x
-
Marchal F. Sialendoscopy. In: Myers EN, Ferris RL, eds. Salivary Gland Disorders. Springer; 2007:ch 6.
-
Yu C, Zheng L, Yang C, Shen N. Causes of chronic obstructive parotitis and management by sialoendoscopy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(3):365-371. https://doi.org/10.1016/j.tripleo.2007.08.008
-
Fritsch MH. Sialendoscopy and lithotripsy: literature review. Otolaryngol Clin North Am. 2009;42(6):915-926. https://doi.org/10.1016/j.otc.2009.09.001
-
Chikamatsu K, Shino M, Fukuda Y, et al. Recurring bilateral parotid gland swelling: two cases of sialodochitis fibrinosa. J Laryngol Otol. 2006;120(4):330-333. https://doi.org/10.1017/S0022215106000296
-
Chuangqi Y, Chi Y, Lingyan Z. Sialendoscopic findings in patients with obstructive sialadenitis: long-term experience. Br J Oral Maxillofac Surg. 2013;51(4):337-341. https://doi.org/10.1016/j.bjoms.2012.07.013
-
Gür H, Özcan C, Güven O, et al. Diagnostic and therapeutic value of sialendoscopy in a patient with Kussmaul disease: A case report. B-ENT. 2023;19(3):184-187. https://doi.org/10.5152/B-ENT.2023.221087
-
Kussmaul I. Anfallweise auftertende Speichelgeschwulst [Salivary tumors that appear in fits and starts]. Berlin Klin Wschr. 1879;15.
-
Tymofieiev OO. Non-neoplastic diseases of the salivary glands. In: Tymofieiev OO, ed. Surgical Dentistry and Maxillofacial Surgery. Vol 2. Marchenko TV; 2025:chap 2. Ukrainian.
-
Yoshioka Y, Makino K, Sakoda K, et al. Sialodochitis fibrinosa of the parotid glands: A case report. Kōkū Intōka (Stomato-pharyngology).1997;9:409-416.
-
Pollak N, Templer JW, Esebua M, et al. Episodic painful parotid swelling caused by sialodochitis with eosinophilic inflammation: a new entity. Otolaryngol Head Neck Surg. 2009;140(1):132-133.
-
Shimada T, Okano H, Hisa Y. A case of severe dilatation of the parotid duct due to fibrinous sialodochitis. Acta Otolaryngol. 2006;126(10):1112-1114.
-
Tsuchiya A, Aizawa N, Sato K, Takahashi S. Three cases of sialodochitis fibrinosa. Kōkū Intōka (Stomato-pharyngology). 2012;25(2):173-177.
-
Motosugi H, Itoh H, Tachibana M, et al. Two cases of sialodochitis fibrinosa. Kōkū Intōka (Stomato-pharyngology). 1998;10(3):345-349.
-
Hayashi K, Onda T, Ohata H, et al. Case of suspected sialodochitis fibrinosa (Kussmaul's disease). Bull Tokyo Dent Coll. 2016;57(2):91-96. https://doi.org/10.2209/tdcpublication.2015-0028
-
Salazar P, Celestin J. M104 Sialodochitis fibrinosa: an uncommon and possibly allergic disease of the salivary glands. Ann Allergy Asthma Immunol. 2020;125(5 Suppl):S67. https://doi.org/10.1016/j.anai.2020.08.219
-
Jung HS, Chang IS, Kim JY, et al. Role of ultrasonography in the diagnosis and management of chronic recurrent sialadenitis with sialendoscopy. J Korean Assoc Oral Maxillofac Surg. 2025;51(2):117-123. https://doi.org/10.5125/jkaoms.2025.51.2.117
-
Pang SL, Lo AWI, Wang R, Su YX. Sialendoscopic removal of metastatic adenocarcinoma in a mucous plug from Stensen’s duct. Int J Oral Maxillofac Surg. 2023;52(10):1025-1027. https://doi.org/10.1016/j.ijom.2023.01.011
-
Steck JH, Stabenow E, Volpi EM, Vasconcelos EC. The learning progression of diagnostic sialendoscopy. Braz J Otorhinolaryngol. 2016;82(2):170-176. doi:10.1016/j.bjorl.2015.10.007
-
Demidov VH, Ripolovska OV. How multiple the submandubular gland sialoliths can be? J Diagn Treat Oral Maxillofac Pathol. 2019;3(7):174-175. https://doi.org/10.23999/j.dtomp.2019.7.2
-
Bodner L. Parotid sialolithiasis. J Laryngol Otol. 1999;113(3):266-267. https://doi.org/10.1017/s0022215100143750
-
Nikulin DS, Fesenko II, Cherniak OS. Sialoliths in ipsilateral Bartholin`s and Wharton`s duct: the first clinical and ultrasound report. J Diagn Treat Oral Maxillofac Pathol 2020;4(7):112–8. https://doi.org/10.23999/j.dtomp.2020.7.2
-
Liao LJ, Hsiao JK, Hsu WC, Wang CP. Sublingual gland sialolithiasis: a case report. Kaohsiung J Med Sci. 2007;23(11):590-593. https://doi.org/10.1111/j.2410-8650.2007.tb00003.x
-
Huang HK, Hwang MJ, Chiang CP, Jin YT. Sialoliths in the minor salivary glands of the upper lip. J Dent Sci. 2023;18(3):1392-1394. https://doi.org/10.1016/j.jds.2023.01.032
-
Tanna N, Koshal S. Rare sialoliths of the minor salivary glands: a case series and review of the literature. Oral Surgery. 2016;9(2):107-112. https://doi.org/10.1111/ors.12164
-
Ben Lagha N, Alantar A, Samson J, Chapireau D, Maman L. Lithiasis of minor salivary glands: current data. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(3):345-348. https://doi.org/10.1016/j.tripleo.2004.12.023
-
Zenk J, Koch M, Klintworth N, et al. Sialendoscopy in the diagnosis and treatment of sialolithiasis: a study on more than 1000 patients. Otolaryngol Head Neck Surg. 2012;147(5):858-863. https://doi.org/10.1177/0194599812452837
-
Tanaka N, Ichinose S, Adachi Y, et al. Ultrastructural analysis of salivary calculus in combination with x-ray microanalysis. Med Electron Microsc. 2003;36(2):120-126. https://doi.org/10.1007/s00795-002-0210-z
-
Iwanaga J, Tubbs RS, Kitagawa N, et al. Facial landmark-based localization of the parotid duct: a cadaveric study with ultrasonographic feasibility assessment. Sci Rep. 2026;16(1):11082. https://doi.org/10.1038/s41598-026-41701-1
-
Amiel T, Shauly O, Istoyler EG, et al. The anatomical pattern of ductal arborization in parotid glands using cone-beam computerized sialography. Clin Anat. 2024;37(8):878-885. https://doi.org/10.1002/ca.24136
-
Hong KH, Yang YS. Sialolithiasis in the sublingual gland. J Laryngol Otol. 2003;117(11):900-902. https://doi.org/10.1258/002221503322542971
-
Choi J, Kim IK, Oh NS. Multiple sialoliths in sublingual gland: report of a case. Int J Oral Maxillofac Surg. 2002;31(5):562-563. https://doi.org/10.1054/ijom.2002.0253
-
Lee JH, No YH, Cha YW, Kim SW. A case of multiple sialoliths in sublingual gland misdiagnosed as sialoliths in submandibular gland. Korean J Otolaryngol-Head Neck Surg. 2011;54(1):81-84. https://doi.org/10.3342/kjorl.2011.54.1.81
-
Marchal F, Chossegros C, Faure F, et al. Lithiases et sténoses salivaires. Une classification pratique des pathologies non tumorales [Salivary stones and stenosis. A comprehensive classification]. Rev Stomatol Chir Maxillofac. 2009;110(1):e1-e4. https://doi.org/10.1016/j.stomax.2008.10.002
-
Tymofieiev OO, Cherniak OS. Ultrasound in the detection of floating sialoliths. J Diagn Treat Oral Maxillofac Pathol. 2019;3(8):196-197. https://doi.org/10.23999/j.dtomp.2019.8.2
-
Lustmann J, Regev E, Melamed Y. Sialolithiasis. A survey on 245 patients and a review of the literature. Int J Oral Maxillofac Surg. 1990;19(3):135-138. https://doi.org/10.1016/s0901-5027(05)80127-4
-
Carlson ER. Diagnosis and management of salivary gland infections. Oral Maxillofac Surg Clin North Am. 2009;21(3):293-312. https://doi.org/10.1016/j.coms.2009.04.004
-
Terraz S, Poletti PA, Dulguerov P, et al. How reliable is sonography in the assessment of sialolithiasis?. AJR Am J Roentgenol. 2013;201(1):W104-W109. https://doi.org/10.2214/AJR.12.9383
-
Hoffman HT, Koch M, Witt RL, et al. Proposal for standardized ultrasound analysis of the salivary glands: Part 1 submandibular gland. Laryngoscope Investig Otolaryngol. 2024;9(1):e1224. https://doi.org/10.1002/lio2.1224
-
Howlett DC, Alyas F, Wong KT, et al. Sonographic assessment of the submandibular space. Clin Radiol. 2004;59(12):1070-1078. https://doi.org/10.1016/j.crad.2004.06.025
-
Orloff LA, Hwang HS, Jecker P. The role of ultrasound in the diagnosis and management of salivary disease. Oper Tech Otolaryngol Head Neck Surg. 2009;20(2):129-135. https://doi.org/10.1016/j.otot.2009.02.004
-
Hoffman H, ed. Salivary ultrasound sonopalpation for stone favorable for transoral removal. Iowa Head and Neck Protocols. October 30, 2017. Accessed January 05, 2026. https://iowaprotocols.medicine.uiowa.edu/protocols/salivary-ultrasound-sonopalpation-stone-favorable-transoral-removal
-
Schapher M, Goncalves M, Mantsopoulos K, Iro H, Koch M. Transoral ultrasound in the diagnosis of obstructive salivary gland pathologies. Ultrasound Med Biol. 2019;45(9):2338-2348. https://doi.org/10.1016/j.ultrasmedbio.2019.05.019
-
Koch M, Schapher M, Goncalves M, Iro H, Mantsopoulos K. Simultaneous application of ultrasound and sialendoscopy: experience in the management of stenosis and other non-sialolithiasis-related salivary gland disorders. Eur Rev Med Pharmacol Sci. 2020;24(5):2196-2204. https://doi.org/10.26355/eurrev_202003_20485
-
Lystad H, Yu E, Subramony R. Parotid sialolithiasis diagnosed on point of care ultrasound (POCUS). POCUS J. 2025;10(1):104-106. https://doi.org/10.24908/pocusj.v10i01.18657
-
Hosokawa T, Tanami Y, Sato Y, et al. Clinical audit of ultrasonography for detecting sialoliths in the submandibular gland in paediatric patients: A comparison to computed tomography and magnetic resonance imaging. Australas J Ultrasound Med. 2023;27(1):19-25. https://doi.org/10.1002/ajum.12370
-
Hoffmann B. Sonographic bedside detection of sialolithiasis with submandibular gland obstruction. Am J Emerg Med. 2011;29(5): 574.e5-574.e7. https://doi.org/10.1016/j.ajem.2010.05.020
-
Koch M, Sievert M, Iro H, Mantsopoulos K, Schapher M. Ultrasound in inflammatory and obstructive salivary gland diseases: Own experiences and a review of the literature. J Clin Med. 2021;10(16):3547. https://doi.org/10.3390/jcm10163547
-
Huang F, Caton R, Colla J. Point-of-care ultrasound diagnosis of acute sialolithiasis with sialadenitis. Clin Pract Cases Emerg Med. 2017;1(4):437-438. https://doi.org/10.5811/cpcem.2017.7.34907
-
Pniak T, Štrympl P, Staníková L, et al. Sialoendoscopy, sialography, and ultrasound: a comparison of diagnostic methods. Open Med (Wars). 2016;11(1):461-464. Published 2016 Nov 26. https://doi.org/10.1515/med-2016-0081
-
Hoffman HT, Pagedar NA. Ultrasound-guided salivary gland techniques and interpretations. Atlas Oral Maxillofac Surg Clin North Am. 2018;26(2):119-132. https://doi.org/10.1016/j.cxom.2018.04.001
-
Chung MK, Jeong HS, Ko MH, et al. Pediatric sialolithiasis: what is different from adult sialolithiasis? Int J Pediatr Otorhinolaryngol. 2007;71(5):787-791. https://doi.org/10.1016/j.ijporl.2007.01.019
-
Kim DH, Song WS, Kim YJ, Kim WD. Parotid sialolithiasis in a two-year-old boy. Korean J Pediatr. 2013;56(10):451-455. https://doi.org/10.3345/kjp.2013.56.10.451
-
Benson BW. Salivary gland diseases. In: White SC, Pharoah MJ, eds. Oral Radiology: Principles and Interpretation. 7th ed. Elsevier; 2014:chap 29.
-
Kraaij S, Karagozoglu KH, Forouzanfar T, et al. Salivary stones: symptoms, aetiology, biochemical composition and treatment. BDJ. 2014;217(11):E23. doi:10.1038/sj.bdj.2014.1054
-
Mostafavi Tabatabaee R, Mostafavi Tabatabaee R, Sanatkhani M. Salivary megaliths: a literature review of giant salivary sialoliths larger than 30 mm. J Pharm Res Int. 2019;29(4):1-17. https://doi.org/10.9734/jpri/2019/v29i430245
-
Nozhenko OA, Savchuk LA, Zaritska VI, et al. Phleboliths, not sialoliths: a report of submandibular gland arteriovenous malformation with numerous calcifications: analysis of cine images and literature review for the 54 years. J Diagn Treat Oral Maxillofac Pathol. 2023;7(7):63-86. https://doi.org/10.23999/j.dtomp.2023.7.1
-
Teymoortash A, Ramaswamy A, Werner JA. Is there evidence of a sphincter system in Wharton's duct? Etiological factors related to sialolith formation. J Oral Sci. 2003;45(4):233-235. https://doi.org/10.2334/josnusd.45.233
-
Beahm DD, Peleaz L, Nuss DW, et al. Surgical approaches to the submandibular gland: a review of literature. Int J Surg. 2009;7(6):503-509. https://doi.org/10.1016/j.ijsu.2009.09.006
-
Tymofieiev OO. Diseases of the Salivary Glands. VNTL-Klasyka; 2007. Ukrainian.
-
Savchuk LA, Fesenko II. Obstructive submandibular sialadenitis complicated with severe neck phlegmon: transcutaneous removal of sialolith with a flow of pus: literature review of extraoral complications. J Diagn Treat Oral Maxillofac Pathol. 2021;5(11):125-134. https://doi.org/10.23999/j.dtomp.2021.11.1
-
Markiewicz MR, Margarone JE 3rd, Tapia JL, Aguirre A. Sialolithiasis in a residual Wharton’s duct after excision of a submandibular salivary gland. J Laryngol Otol. 2007;121(2):182-185. https://doi.org/10.1017/s0022215106003525
-
Su LW, Sun H, Zhang HY, Wu Y. Large recurrent sialoliths in a residual Wharton duct after sialoadenectomy: Two case reports and literature review. Medicine (Baltimore). 2025;104(2):e41231. https://doi.org/10.1097/md.0000000000041231
-
Ahmed SS, Abid S, Al-Thobaiti Y, et al. Longstanding unrecognized wooden foreign bodies in oro-facial region, report of three cases. Am J Public Health Res. 2015;3(4):157-161. https://doi.org/10.12691/ajphr-3-4-5
-
Gill AS, Kieliszak CR, Joshi AS. Sialendoscopy as a management tool in patients with foreign body impaction of the salivary gland. Am J Otolaryngol. 2016;37(4):369-371. https://doi.org/10.1016/j.amjoto.2016.02.008
-
Zheng DN, Xu XY, Ling XT, Liu DG. Stensen’s duct penetration and sialolith formation: a rare complication of thread lifting surgery. J Stomatol Oral Maxillofac Surg. 2025;126(5S):102489. https://doi.org/10.1016/j.jormas.2025.102489
-
Luo WD, Jia YP, Gong J, Zhao Q. Unusual foreign body spontaneously discharged from the submandibular gland: A case report. J Clin Ultrasound. 2022;50(2):243-246. https://doi.org/10.1002/jcu.23045
-
Oz C, Kapi E, Erkan SO, Külahçi Ö. Etiology of a rare intraglandular foreign body in the parotid gland: Vegetable nidus. Turk J Plast Surg. 2022;30(3):76-78. https://doi.org/10.4103/tjps.tjps_12_22
-
Sato K, Umeno H. Clinical photographs. Fish bone-induced sialolith. Otolaryngol Head Neck Surg. 2009;141(4):539-540. https://doi.org/10.1016/j.otohns.2009.05.002
-
Yoshida M, Yamamoto K, Shimasue H, et al. A case of acute submandibular sialadenitis caused by a fish bone that strayed into the submandibular gland duct. Oral Sci Int. 2024;21(2):123-127. https://doi.org/10.1002/osi2.1217
-
Smith AB, Jones CD. Ultrasound diagnosis and sialadenectomy confirming a mandibular salivary gland vegetative foreign body and chronic sialadenitis in a dog. J Am Vet Med Assoc. 2024;264(3):112-115. https://doi.org/10.1016/j.javma.2026.01.002
-
Oliaei S. Are there ways to prevent salivary stones? Instagram. February 18, 2026. Accessed June 19, 2026. https://www.instagram.com/reel/DU6QOTaDGob/
-
Lee CC, Huang JC, Shin JS, Wu MJ. Tumefactive sludge mimicking gallbladder neoplasm: A case report and review of the literature. J Med Ultrasound. 2018;26(2):103-106. https://doi.org/10.4103/JMU.JMU_19_18
-
Bradley MJ. Salivary glands. In: Ahuja A, Evans R, eds. Practical Head and Neck Ultrasound. Greenwich Medical Media; 2000:ch 2.
-
Aoun G, Maksoud C. Sialolith of unusual size and shape in the anterior segment of the submandibular duct. Cureus. 2022;14(4):e24114. https://doi.org/10.7759/cureus.24114