
Assessment of the Relationship of the Frankfort Horizontal Plane and the Orbitomeatal Line with Attainment of the Natural Head Position
December 28, 2017
https://doi.org/10.23999/j.dtomp.2017.3-4.8
J Diagn Treat Oral Maxillofac Pathol 2017;1:156−63.
Under a Creative Commons license
How to cite this article
Cruz RLA, Gasperini G. Assessment of the relationship of the frankfort horizontal plane and the orbitomeatal line with attainment of the natural head position. J Diagn Treat Oral Maxillofac Pathol 2017;1(3−4):156−63.
Contents: Abstract | Introduction | Matherial and Methods | Results | Discussion | References (23)
ABSTRACT
The diagnosis of dentofacial deformities and the choice of ortho-surgical treatment depend on the correct positioning of the head at the time of registration in 2D or 3D, called the natural head position (NHP). We selected 32 subjects from Arnett class I and obtained their frontal and lateral photographs in NHP to evaluate the relationship and stability between the orbitomeatal line, the Frankfort horizontal plane and the face midline with the true vertical line (TVL) and the true horizontal line (THL). Mean and standard deviation of angulation were obtained for all cited variables, with the results leading to the conclusion that the orbitomeatal line and the Frankfort horizontal plane can be used to obtain the NHP in an individualized way.
Introduction
Facial esthetics can influence psychological factors, social development, and the quality of life of patients. The contour of the soft tissue, the skeletal relationships, and the functional occlusion should be considered in the diagnosis and planning of ortho-surgical treatment. Therefore, orthodontic treatment and orthognathic surgery have the objective of correcting facial and skeletal facial discrepancies, and altering the facial profile, in order to achieve satisfactory esthetic and functional results in patients [1].
Anthropomorphic studies of the head for investigation or clinical evaluation require a standard orientation of the skull as a reference. In 1884, the concept that the Frankfort horizontal plane could be used as the horizontal intracranial reference was adopted, which served as a guide for the correct positioning of the head. Since 1950, the perception that the Frankfort plane may not always be horizontal when the natural head position (NHP) is adopted has resulted in a greater interest in obtaining the NHP for cephalometric measurements [2-4].
The NHP was first described in 1862 and occurs when a patient is looking at a distant point at eye level, which implies that the visual axis is horizontal [5]. However, it was only during the 1950s that the term “natural head position” was introduced into orthodontic assessment, considered to be a stable, reproducible position that seems to correlate better with the actual craniofacial morphology, in addition to being related to future patterns of skeletal growth and type of respiration [6].
Obtaining the NHP has the advantage that it can be associated with extra-cranial reference lines for cephalometric analysis [3]. According to Arnett and McLaughlin [7], these references are the true vertical line that is drawn along the subnasal area perpendicular to the NHP, and the true horizontal line that is parallel to the ground.
NHP and natural head posture are terms that are constantly used as synonyms. However, more specifically, the NHP determines the relationship of the head to the TVL and the natural posture of the head determines the relationship of the head to the cervical spine [3, 8].
The Frankfort horizontal plane (porion-orbital) is used to obtain cephalograms oriented parallel to the ground. The technique is reproducible and provides a clear view of cephalograms, with few projection errors, but can modify the patient’s natural posture and consequently also cause variations in the NHP of each person [7, 9].
When taking cranial radiographs, there are other reference lines that can be used in addition to the Frankfort horizontal plane. The orbitomeatal line, located between the outer corner of the eye and the midpoint of the patient’s tragus, is one of them. Used for the clinical positioning of the patient prior to radiography, it forms an angle of approximately 10 degrees with the Frankfort horizontal plane [10-13].
The objectives of this study are to evaluate the relationships of the Frankfort horizontal plane and the orbitomeatal line with the TVL and THL and to evaluate the relationship of the face midline with the TVL, in order to determine whether there is a standard measure to achieve the NHP for all patients.
Materials and Methods
This was a comparative cross-sectional study, approved by the Ethics Committee of the Clinical Hospital of the Federal University of Goiás. It initially involved the evaluation of 85 subjects randomly selected from the community, from June 2016 to December 2016, who were older than 18 years of age and had complete dentition to at least the first molars. Those with a scar in the facial region or a deformity or postural difficulty were excluded.
Frontal and profile photographs of each subject were obtained with a Canon EOS Rebel T5 DSLR digital camera, 18MP, in the same environment and by the same operator, using a white background and a plumb representing the TVL. At the moment of photographing, the subjects were standing with a NHP, which was obtained by directing them to look at the image of their own pupils in a mirror placed 2 m away, with shoulders and head relaxed. The camera was positioned on a tripod, 2 m away from each subject, at face level, with a central focus centered on the point of the greatest prominence of the zygomatic bone in the profile photographs and at the tip of the nose in the frontal photographs. The operator did not perform accommodation maneuvers or postural modification on the subjects.
Markings with a blue tip pen were made on the following anatomical landmarks of the subject:
-
Mean point of the distance between the medial corners of the eyes and the point located in the upper lip filtrum, for the facial midline (Fig 1A, B).
-
Orbital craniometric point and superior point of the external acoustic meatus, for the Frankfort horizontal plane.
-
Skin point of the outer corner of the eye and tragus midpoint for orbitomeatal line tracing (Fig 2A, B).


FIGURE 1A. (A) Markings (dots) in the mean point of the distance between the medial corners of the eyes and the point located in the upper lip filtrum. (B) Tracing of the facial midline (red line) and the TVL (black line).
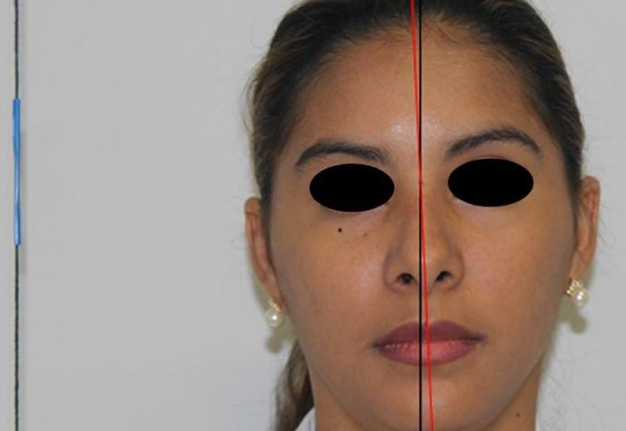
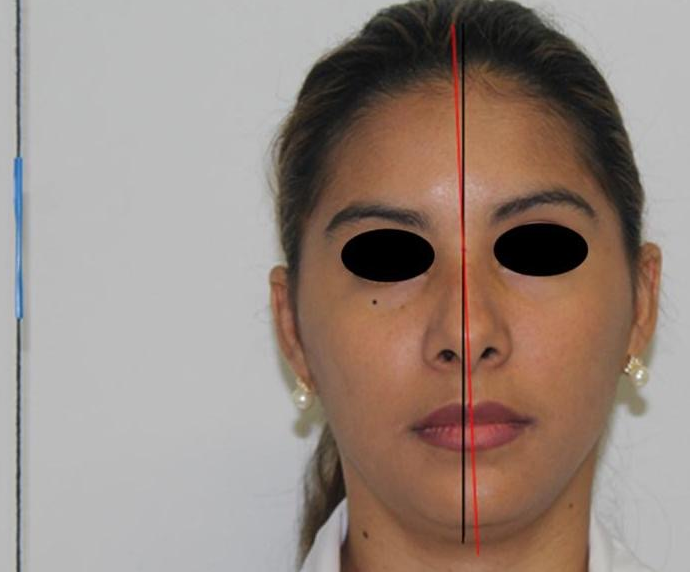
FIGURE 1B. (A) Markings (dots) in the mean point of the distance between the medial corners of the eyes and the point located in the upper lip filtrum. (B) Tracing of the facial midline (red line) and the TVL (black line).

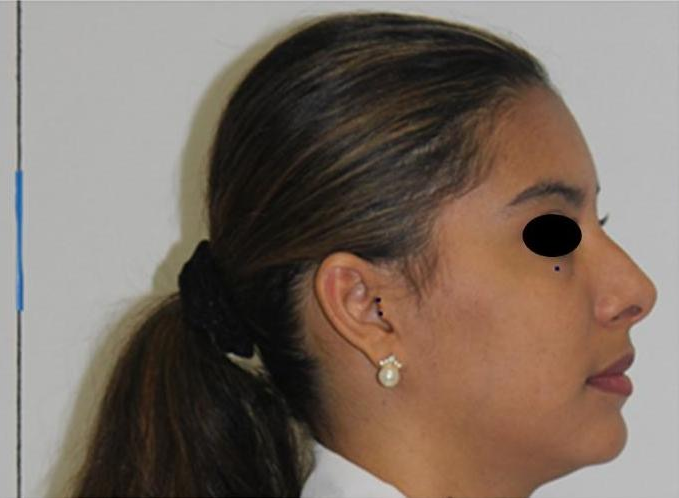
FIGURE 2A. (A) Markings (dots) in the orbital craniometric point, the superior point of the external acoustic meatus, the skin point of the outer corner of the eye and the tragus midpoint. (B) Tracing of the orbitomeatal line (upper line) and the Frankfort horizontal plane (lower line).
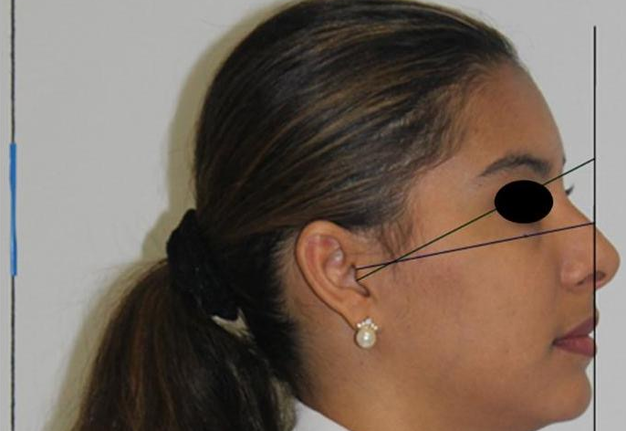

FIGURE 2B. (A) Markings (dots) in the orbital craniometric point, the superior point of the external acoustic meatus, the skin point of the outer corner of the eye and the tragus midpoint. (B) Tracing of the orbitomeatal line (upper line) and the Frankfort horizontal plane (lower line).
All photographs included a 7-cm marking device on the plumb and the distance between the tragus and the outer corner of the eye was also recorded to aid in reproducing the original size of the profile photograph at the time of the computerized analysis of data. At the end of the recording, all photographs were scanned and analyzed in the AutoCAD® measurement and drawing program, version 2010.
The orbitomeatal line, the Frankfort horizontal plane and the midline of the face were identified by using tracing and angulation tools. The TVL was identified by transferring the line formed by the plumb, passing through the middle intercantal point in the frontal photograph, and passing through the subnasal point in the profile photo.
Arnett’s cephalometric analysis of soft tissue (CAST) was performed and it was determined that only 32 subjects from the 85 chosen initially had the Arnett Class I-compatible facial profile, which is considered to be the most esthetic and harmonious; therefore, 53 subjects were excluded from the final sample.
The following angles were obtained in the AutoCAD® program, version 2010:
- Profile photograph:
a. Angle formed between orbitomeatal line and true vertical line (OML-TVL).
b. Angle formed between Frankfort horizontal plane and true vertical line (FHP-TVL).
c. Angle formed between orbitomeatal line and true horizontal line (OML-THL).
d. Angle formed between Frankfort horizontal plane and true horizontal line (FHP-THL).
e. Angle formed between orbitomeatal line and Frankfort horizontal plane (OML-FHP).
-
Frontal photograph:
a. Angle formed between face midline and true vertical line (FML-TVL).
A sample calculation was performed to compare the means of all angulation variables and the CAST variables that had been calculated between male (n = 11) and female (n = 21) subjects; the calculation was of the two-tailed type, with absolute error of 5%, and effect of the delineation of 3.0 (determined from data of the present study) totaling test power of 100%. The analysis was performed using G * Power ® software version 3.1.9.2.
To perform the statistical analysis, the collected data were tabulated and stored using a spreadsheet, specially developed for this research, of the Microsoft Office Excel® program, version 2013. Statistical analysis of the variables was performed in the statistical package STATA® version 12.0.
For descriptive analysis, continuous variables were expressed as mean, standard deviation, and 95% confidence interval of the mean. Then, the normality of the continuous variables was tested using the Shapiro–Wilk test. Subsequently, we compared the means by classifying subjects by sex (male/female) using the Student’s t or Mann–Whitney test. Statistically significant data were those that presented a P value <0.05.
A simulation was performed with the values obtained in a subject using the AutoCAD® software, version 2010, by adapting the position of the photograph to the mean angulation obtained for OML-TVL and FHP-TVL, and to the higher and lower recorded values of both variables to determine the true clinical impact of these variables in the antero-posterior projection of important structures for the cephalometric analysis of soft tissue (Figs 3 and 4).
Results
The cephalometric analysis of soft tissue performed on the 32 subjects was consistent with the values established for Arnett Class I, where prominence of the upper lip (UL), lower lip (LL), and soft-tissue pogonium (PG) in relation to the TVL expresses a more harmonic and esthetic facial profile (Table 1).
The angulation values obtained in the analysis of the variables showed different amplitudes between the lowest and highest values recorded (Table 2).
The results of the statistical analysis on the achievement of normality in the male and female genders showed that there were no statistically significant differences when comparing the values of most of the angulation measures between the two genders. When the t-test was performed with a significance level of 0.05, it was found that the only measures that showed a notable difference between males and females were the relationship of upper lip and TVL and the relationship of lower lip and TVL, but both values remained within parameters considered normal by Arnett (Table 3).
The simulation performed with the photograph of a subject showed that the different angulation values of the OML-TVL and FHP-TVL variables can cause a small but important difference at the time of the cephalometric analysis of soft tissue when the patient is positioned according to the data obtained in this study (Table 4).
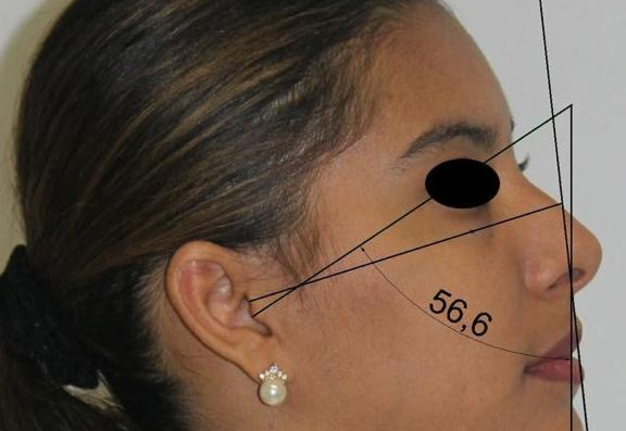
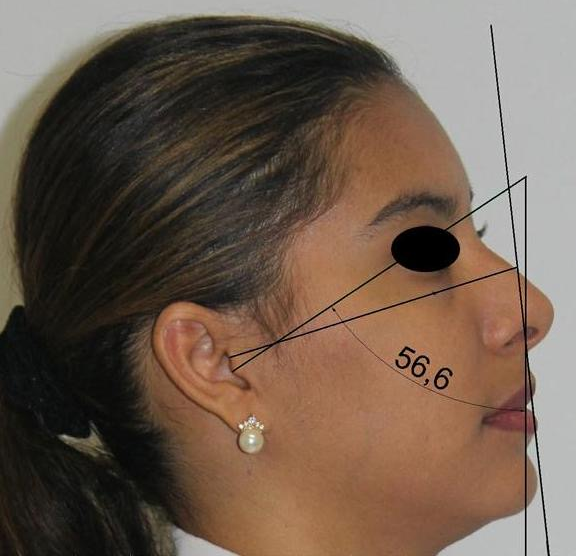
FIGURE 3A. Simulation performed with the values obtained in OML-TVL. (A) Adapting the position of the photograph to the lower value recorded. (B) Adapting the position of the photograph to the higher value recorded.
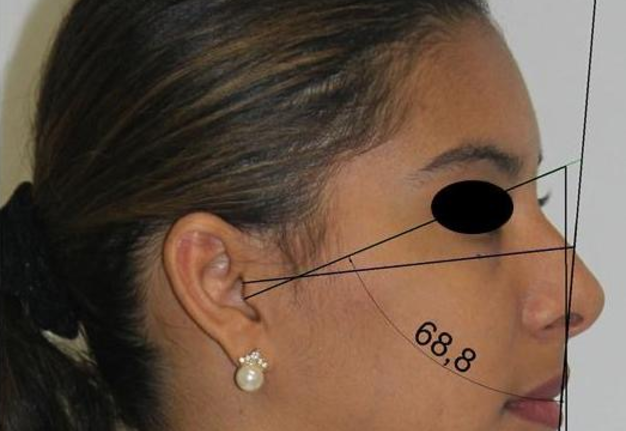
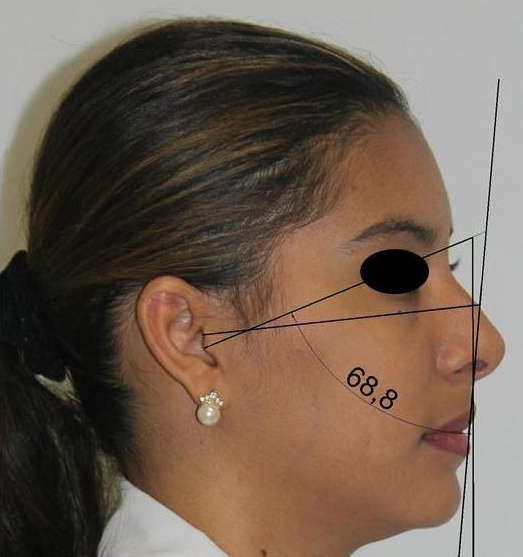
FIGURE 3B. Simulation performed with the values obtained in OML-TVL. (A) Adapting the position of the photograph to the lower value recorded. (B) Adapting the position of the photograph to the higher value recorded.
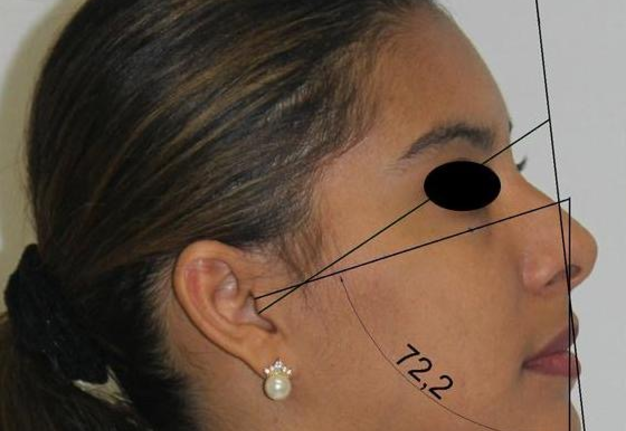
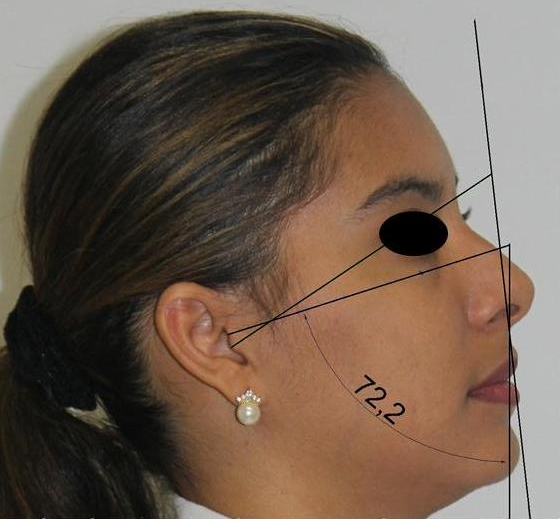
FIGURE 4A. Simulation performed with the values obtained in FHP-TVL. (A) Adapting the position of the photograph to the lower value recorded. (B) Adapting the position of the photograph to the higher value recorded.
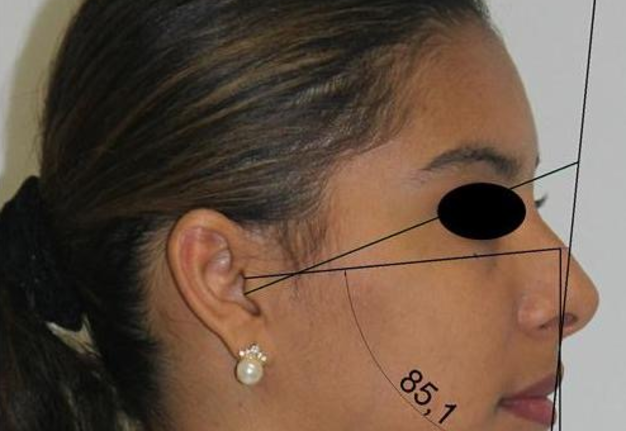
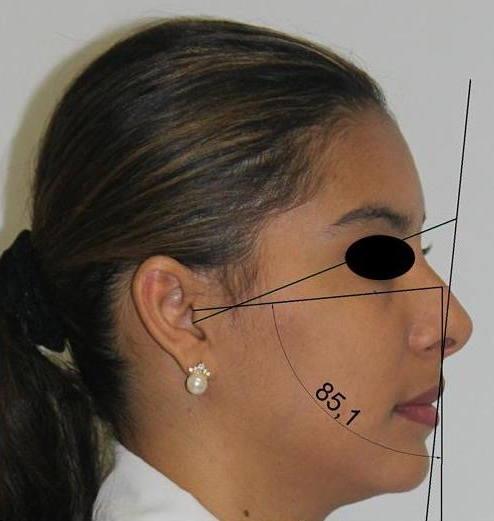
FIGURE 4B. Simulation performed with the values obtained in FHP-TVL. (A) Adapting the position of the photograph to the lower value recorded. (B) Adapting the position of the photograph to the higher value recorded.
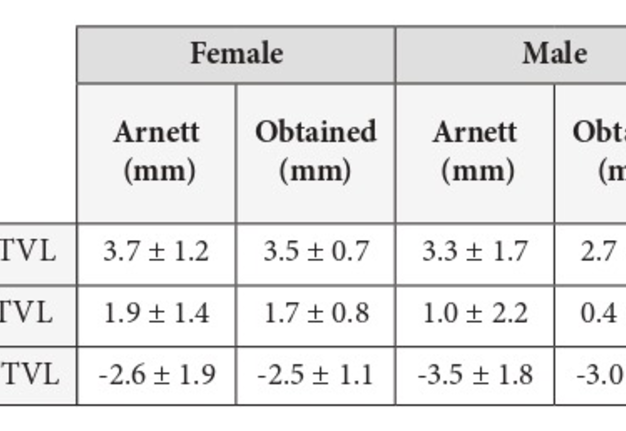
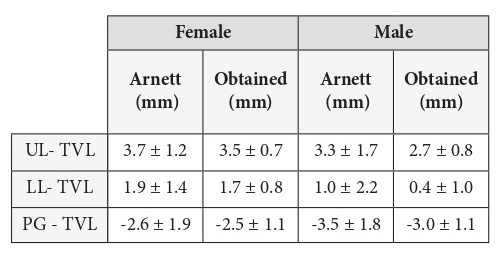
TABLE 1. Mean and standard deviation in Arnett’s CAST and in this study.
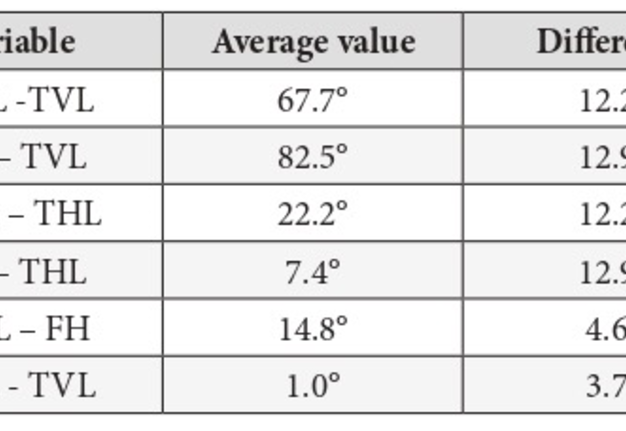
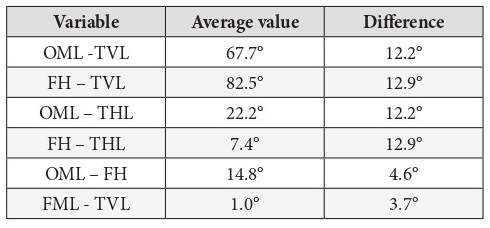
TABLE 2. Angulation values obtained in the analysis of the variables and difference between the lowest and highest values recorded.
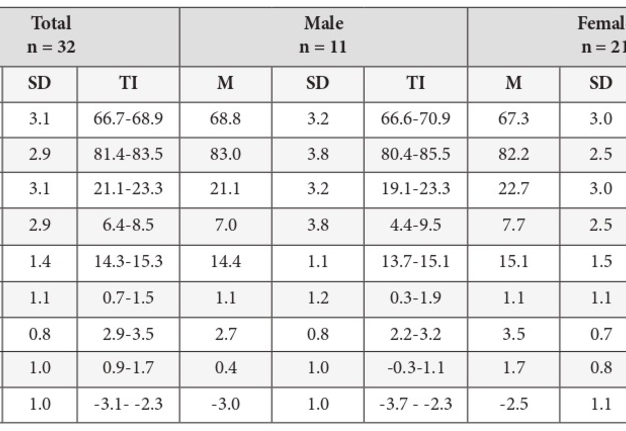
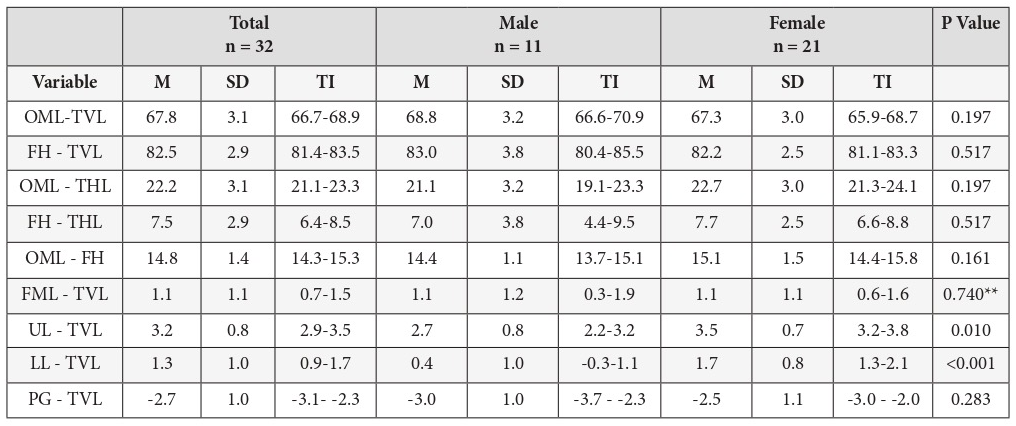
TABLE 3. Results of the statistical analysis showing mean, standard deviation and trust interval for every variable analyzed.
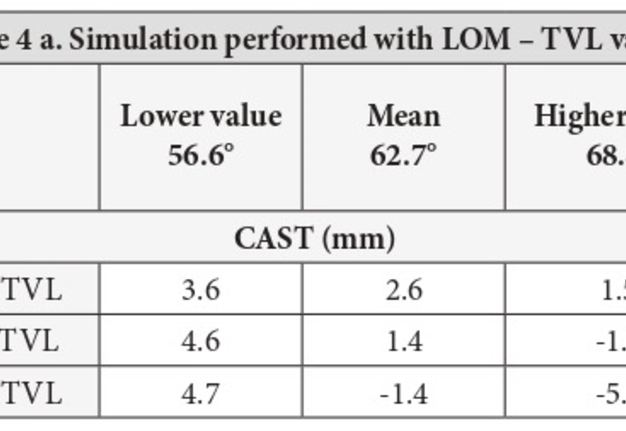
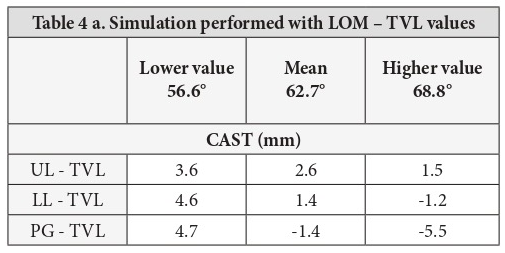
TABLE 4A. Results of the simulation performed with the photograph of a subject.
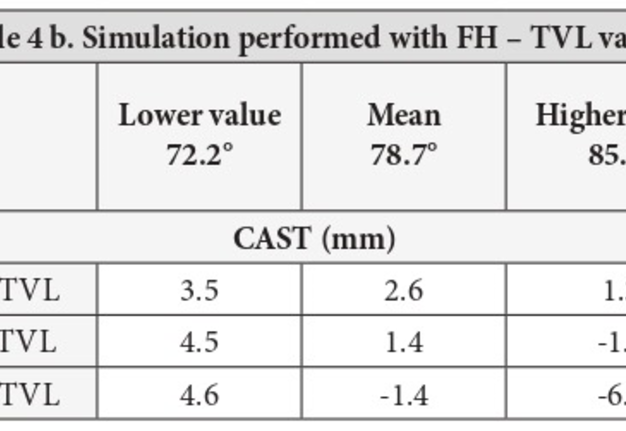
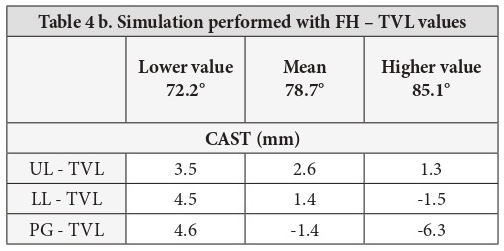
TABLE 4B. Results of the simulation performed with the photograph of a subject.
Discussion
The Frankfort horizontal plane is one of the clinical cephalometric references used more frequently to obtain the NHP. Upon performing teleradiography, the patient is positioned in the cephalostat with the Frankfort horizontal plane, parallel to the ground, which means that, in the image examination, the Frankfort horizontal plane can be traced parallel to the THL [10]. However, in 1993, Arnett and McLaughlin [7] reported that no person has the Frankfort horizontal plane parallel to the ground and there may be patients in the NHP, but with the Frankfort horizontal plane tilted up or down. It is for this reason that the objective of this study was to evaluate the NHP as a better reference related to the craniofacial morphology of subjects.
Obtaining the NHP can be achieved in different ways. Verma et al in 2012 [3] mentioned in their work the study by Solow and Tallgren performed in 1971, in which the patient was asked to walk, perform downward oscillations of the head back and forth until reaching the standing position of “self-equilibrium” and then look at the reflection of his eyes in a mirror 200 cm away. In 1988, Cooke and Wei [14] studied and compared the previous method with another method in which no external reference was used and concluded that reproducibility was better with the mirror method (1.9°) than without it (2.7°). The study by Bister et al in 2002 [15], contradicted previous ones by eliminating the previous procedures of walking and oscillation of the patient’s head. The operator was allowed to interfere and repeat the procedure if the patient’s head was clearly not in the NHP. These authors found reproducibility of 1.4°. In 2015, Tian et al [16] compared the previous methods and added a last method of obtaining the NHP called “estimated position,” and the positioning criteria were that there could be no flexion or extension of the head when observing the side view of the subject, and there could be no obvious inclination from head to the sides when looking at the subject from the front, finding in this method greater reproducibility with a value of 0.9° when compared with the mirror method. In carrying out this study, we opted for the method of Bister et al reported in 2002 [15], using the mirror method without previous oscillatory movements, but contrary to the author’s guidelines there was no interference by the operator, in order to evaluate the subject’s estimated position when positioning for photography as proposed by Tian et al (2015) [16].
Damstra et al (2010) [6] emphasized the importance of recording and studying the NHP in the three planes of space and, from this, Weber et al (2013) [17] stated that the natural position of the head and the inclinations in the coronal axis of individuals are influenced by the vestibulo-ocular and vestibulospinal reflexes, demonstrating that there is less variability of inclination in the coronal axis than in the sagittal axis. To complement this, Liu et al (2015) [18] reported that the gravitational response of the inner ear causes interaction among the head position, the visual axis, the posture of the head, and the muscles. In this study, an average inclination of 1.1° was found between the face midline and the TVL, with a standard deviation of 1.1°. However, the average OML-TVL was 67.8° with standard deviation of 3.1°, and the average FHP-TVL was 82.5° with standard deviation of 2.9°, demonstrating similarity to the findings of Weber et al (2013) [17], showing that there is less inclination in the coronal axis than in the sagittal axis due to the adequate balance among muscular components, visual axis, and inner ear in a homogeneous sample of participants with a harmonic facial profile.
Ramirez et al (2013) [8] performed a study in which the relationship between FHP and THL was 4.4° in men and 3.1° in women without distinction of facial pattern; a result similar to that was obtained by Cooke and Wei in 1988 [14] in their study of the NHP in Chinese children, which was 5.2° in males and 4° in females, also being performed without distinction of facial pattern in their sample. Both studies contradict the work of Lundström and Lundström (1995) [19], who studied the NHP in 79 British children without specific facial pattern, finding statistically significant differences between the genders in the angle formed by FHP and THL, with values of 2.6° for males and 4.1° for females. The discrepancy of the value obtained for males was higher than in the other studies. In contrast to the studies of these authors, the current study has greater homogeneity of the sample when considering only the Arnett Class I facial pattern in the sample. The result for the same angle in this study has mean values of 7.0° for men and 7.7° for women, showing no significant difference between males and females, which is also an important discrepancy when compared with the values obtained in the cited studies.
Ferragio et al (1993) [20], in a study on craniofacial morphometry, performed evaluations of 108 adult subjects, including 57 men and 51 women, without distinction of facial pattern, by taking frontal and lateral facial photographs. The results obtained when evaluating the angle between the Frankfort horizontal plane and the THL were 13° for men and women who were standing and 5° for men and 8° for women who were sitting. This demonstrates that people hold their heads higher when standing. The present study obtained results differing from these, presenting an average angulation of 7.5° with a standard deviation of 2.9° for men and women who were standing at the time of being photographed. This discrepancy may be related to the homogeneity of the sample in this study when compared with the study by Ferragio et al (1993) [20], which included participants with different facial patterns, who compensated the head position in the photograph.
The orbitomeatal line is a reference used less frequently when positioning for and performing cranial radiography. It was found that this line forms an angle of approximately 10° with the Frankfort horizontal plane when studied in radiographs (10–13). This study evaluates the same angulation, but in photography, and the result shows an average value of 14.8° with a standard deviation of 1.4°.
In 1992, Lundström and Lundström [21] took photographs of 52 subjects aged between 10 and 14 years in the NHP. As in the current study, a vertical line was also recorded, obtained by installing a plumb, representing the TVL. Lundström and Lundström also performed radiographic recording of each subject and demonstrated that the reproducibility of the NHP in studies using photographic and radiographic evaluation was approximately 2°. In 1958, Moorrees and Kean [4] studied the reproducibility of the NHP on radiographs, obtaining results of approximately 1.5°. This contrasts to the findings of Kim et al in 2014 [22], who performed evaluation of the NHP on photographs, but obtained similar results with reproducibility of approximately 2° and standard deviation of less than 1°. From this study, Kim et al (2014) [22] determined that the acceptable standard deviation to be clinically insignificant is 2°.
Therefore, small changes in the protocol to obtain the NHP can have considerable effects on possible facial discrepancies. Similarly, the data analysis of this study demonstrated that the angulation values of OML-TVL and FHP-TVL show standard deviations of 3.1° and 2.9°, respectively, showing values that were slightly higher than the proposed clinically acceptable standard deviation reported by Kim et al in 2014 [22].
Like the present study, many others have investigated the variability of cephalometric planes observed on radiographs, such as the Frankfort horizontal plane, saddle-nasion, or Camper plane, with the THL or the TVL to help determine the NHP. In 2012, Verma et al [3] in their study of NHP concluded that the inclination of all intracranial reference lines is subject to biological variation, and therefore they are unsuitable for meaningful cephalometric analysis. These authors have reported that some patients consistently assume a modified NHP, often in an attempt to mask a Class II or Class III facial pattern. For example, a subject with Class II mandibular retrognathism can usually lean back the head to mask the Class II appearance. It is thus, necessary for the clinician to identify these subjects in order to adjust their head position to the registry of the NHP and thus avoid inappropriate values in the cephalometric analysis of bone and soft tissues. This head position is termed “clinician-determined” and provides a more reliable basis for cephalometric analysis. In 2014, Barbera et al [23] reported the difficulty of using a single plane to correct the position of the head because its location, marking, and angulation may vary between subjects.
This study verified that the NHP varies in each person, so it is an individual and biological characteristic that cannot be obtained by assigning an absolute mean to all patients for the purposes of orthognathic surgery planning. It is known that, by performing the wrong positioning at the time of diagnosis and planning, the final result will also be wrong.
The relationship obtained in this study between the orbitomeatal line and the Frankfort horizontal plane with the TVL and the THL has sufficient stability to be an auxiliary method that guides the positioning of the head in cases of extreme discrepancies. Likewise, the relationship between the midline of the face and the TVL demonstrates stability in the coronal axis at the time of obtaining the NHP, providing a suitable reference for its use when positioning the patient’s head and thus avoiding extreme inclinations.
References (23)
-
Chen CM, Lai S, Tseng YC, Lee KT. Simple technique to achieve a natural head position for cephalography. Br J Oral Maxillofac Surg 2008;46:677─8.
-
Chiu CSW, Clark RKF. Reproducibility of natural head position. J Dent 1991;19:130─1.
-
Verma SK, Maheshwari S, Gautam SN, Prabhat KC, Kumar S. Natural head position: key position for radiographic and photographic analysis and research of craniofacial complex. J Oral Biol Craniofac Res 2012;1:46─9.
-
Moorrees CFA, Kean MR, Natural head position, a basic consideration in the interpretation of cephalometric radiographs. Am J Phys Anthropol 1958;16:213–34.
-
Usumez S, Orhan M. Reproducibility of natural head position measured with an inclinometer. Am J Orthod Dentofacial Orthop 2003;123:451–4.
-
Damstra J, Fourie Z, Ren Y. Simple technique to achieve a natural position of the head for cone beam computed tomography. Br J Oral Maxillofac Surg 2010;48:236─8.
-
Arnett GW, McLaughlin RP. Facial and dental planning for orthodontists and oral surgeons. 1st ed. London: Elsevier/Mosby; 2004.
-
Ramírez DM, Jiménez JC, Ramírez EG, Paniagua HJ, Ruidíaz VC. Discrepancies in cephalometric measurements in relation to natural head position. Rev Mex de Ortodoncia 2013;1:27─32.
-
Cassi D, De Biase C, Tonni I, Gandolfini M, Di Blasio A, Piancino MG. Natural position of the head: review of two-dimensional and three-dimensional methods of recording. Br J Oral Maxillofac Surg 2016;54:233─40.
-
Vinita M. Atlas of roentgenographic positions, Vol. 2, 3rd ed. St. Louis: C. V. Mosby CO; 1967.
-
Jacobi CA, Paris DQ. Textbook of radiologic technology. 6th ed. St. Louis: C. V. Mosby; 1977.
-
Bontrager KL, Lampignano JP. Textbook of radiographic positioning and related anatomy. 8th ed. Philadelphia: Elsevier/Mosby; 2013.
-
Swallow RA, Naylor E, Roebuck EJ, Whitley AS. Clark's Positioning in Radiography. 11 ed. New York: William Heinemann; 1986.
-
Cooke MS, Wei SHY. The reproducibility of natural head posture: a methodological study. Am J Orthod Dentofacial Orthop 1988;93:280–8.
-
Bister D, Edler RJ, Tom DDM, et al. Natural head posture ─ considerations of reproducibility. Eur J Orthod 2002; 24:457–70.
-
Tian K, Li Q, Wang X, Liu X, Wang X, Li Z. Reproducibility of natural head position in normal Chinese people. Am J Orthod Dentofacial Orthop 2015;148:503–10.
-
Weber DW, Fallis DW, Packer MD. Three-dimensional reproducibility of natural head position. Am J Orthod Dentofacial Orthop 2013;143:738–44.
-
Liu XJ, Li QQ, Pang YJ, Tian KY, Xie Z, Li ZL. Modified method of recording and reproducing natural head position with a multicamera system and a laser level. Am J Orthod Dentofacial Orthop 2015;147:781–7.
-
Lundström F, Lundström A. The Frankfort horizontal as a basis for cephalometric analysis. Am J Orthod Dentofacial Orthop 1995;107:537–40.
-
Ferragio VF, Sforza C, Miani A, Tartaglia G. Craniofacial morphometry by photographic evaluations. Am J Orthod Dentofacial Orthop 1993;103:327–37.
-
Lundström F, Lundström A. Natural head position as a basis for cephalometric analysis. Am J Orthod Dentofacial Orthop 1992;101:244–7.
-
Kim DS, Yang HJ, Huh KH, Lee SS, Heo MS, Choi SC, Hwang SJ, Yi WJ. Three-dimensional natural head position reproduction using a single facial photograph based on the POSIT method. J Craniomaxillofac Surg 2014;42:1315–21.
-
Barbera AL, Sampson WJ, Townsend GC. Variation in natural head position and establishing corrected head position. Homo 2014;65:187–200.