
August 31, 2019
https://doi.org/10.23999/j.dtomp.2019.8.2
J Diagn Treat Oral Maxillofac Pathol 2017;3:196−7.
Under a Creative Commons license
HOW TO CITE THIS ARTICLE
Tymofieiev OO, Cherniak OS. Ultrasound in the detection of floating sialoliths. J Diagn Treat Oral Maxillofac Pathol 2019;3(8):196−7.
INSTITUTIONAL REPOSITORY
https://ir.kmu.edu.ua/handle/123456789/729
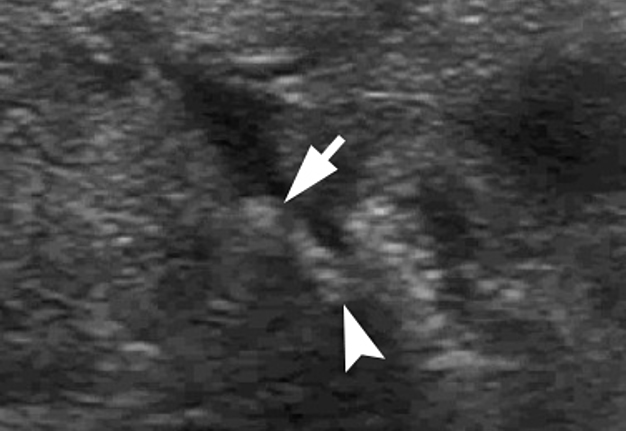
A 36-year-old man with a 3-year history of recurrent salivary colic was referred to a maxillofacial surgery department. Gray scale ultrasound (US) (Video) showed enlarged right submandibular gland, significantly dilated intraglandular duct with two sialoliths (with an artifact of acoustic shadowing) inside, one – floating (Video-Panel A and B, arrow) and another – nonmovable (arrowhead). Left nonsymptomatic normal in size gland (asterisk) is showed at Panel C.
VIDEO. Gray scale ultrasound (US) showed enlarged right submandibular gland, significantly dilated intraglandular duct with two sialoliths (with an artifact of acoustic shadowing) inside, one – floating and another – nonmovable.


VIDEO-PANEL A. Video time 00:01: Gray scale ultrasound (US) shows enlarged right submandibular gland, significantly dilated intraglandular duct with two sialoliths (with an artifact of acoustic shadowing) inside, one – floating (arrow) and another – nonmovable (arrowhead).
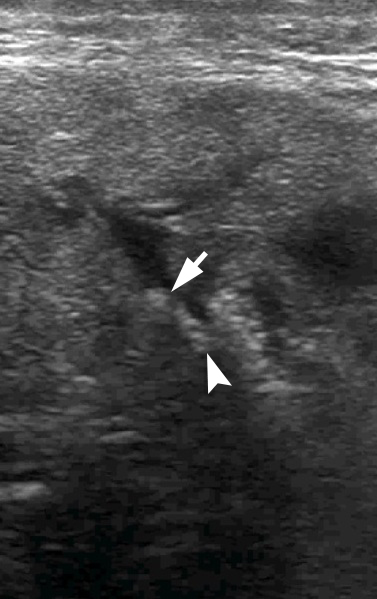
VIDEO-PANEL B. Video time 00:02: Gray scale US shows enlarged right submandibular gland, significantly dilated intraglandular duct with two sialoliths (with an artifact of acoustic shadowing) inside, one – floating (arrow) and another – nonmovable (arrowhead).
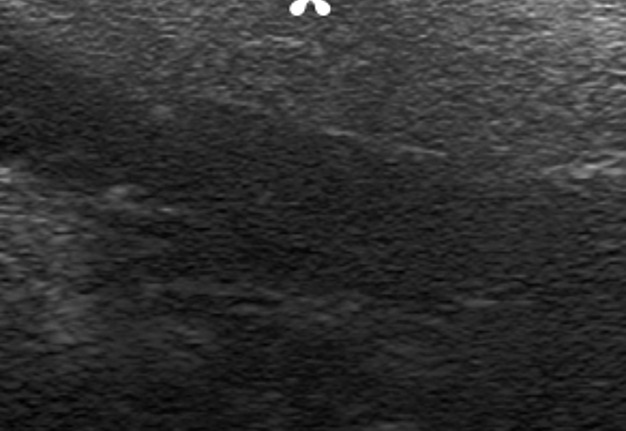

PANEL C. Left nonsymptomatic normal in size gland (asterisk).
The affected gland was excised under general anesthesia due to the diagnosis of chronic submandibular obstructive sialolithiasis. Intraglandular duct contained two yellowish stones, first was an oval form with a pellet surface (Panel D, arrow), second – a round shaped with a smooth surface (Panel D, asterisk) and it was presented at US as a floating sialolith; both are easily crumbled on palpation. As the specimen and intraglandular duct were dissected longitudinally, that`s why dissected intraglandular duct (Panel D, arrowheads) is visible in both parts of the gland. Also, a 1 small calculus (Panel D, curved arrow) was found in the parenchymal ducts. Postoperative period was smooth, and 1-year follow-up after surgery, the patient has no complaints. ■ DTJournal.org
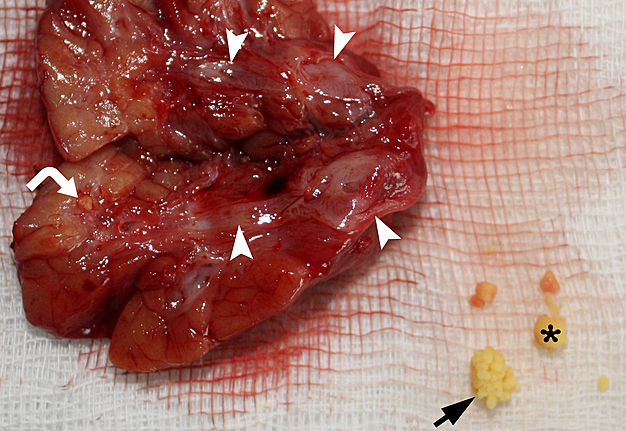
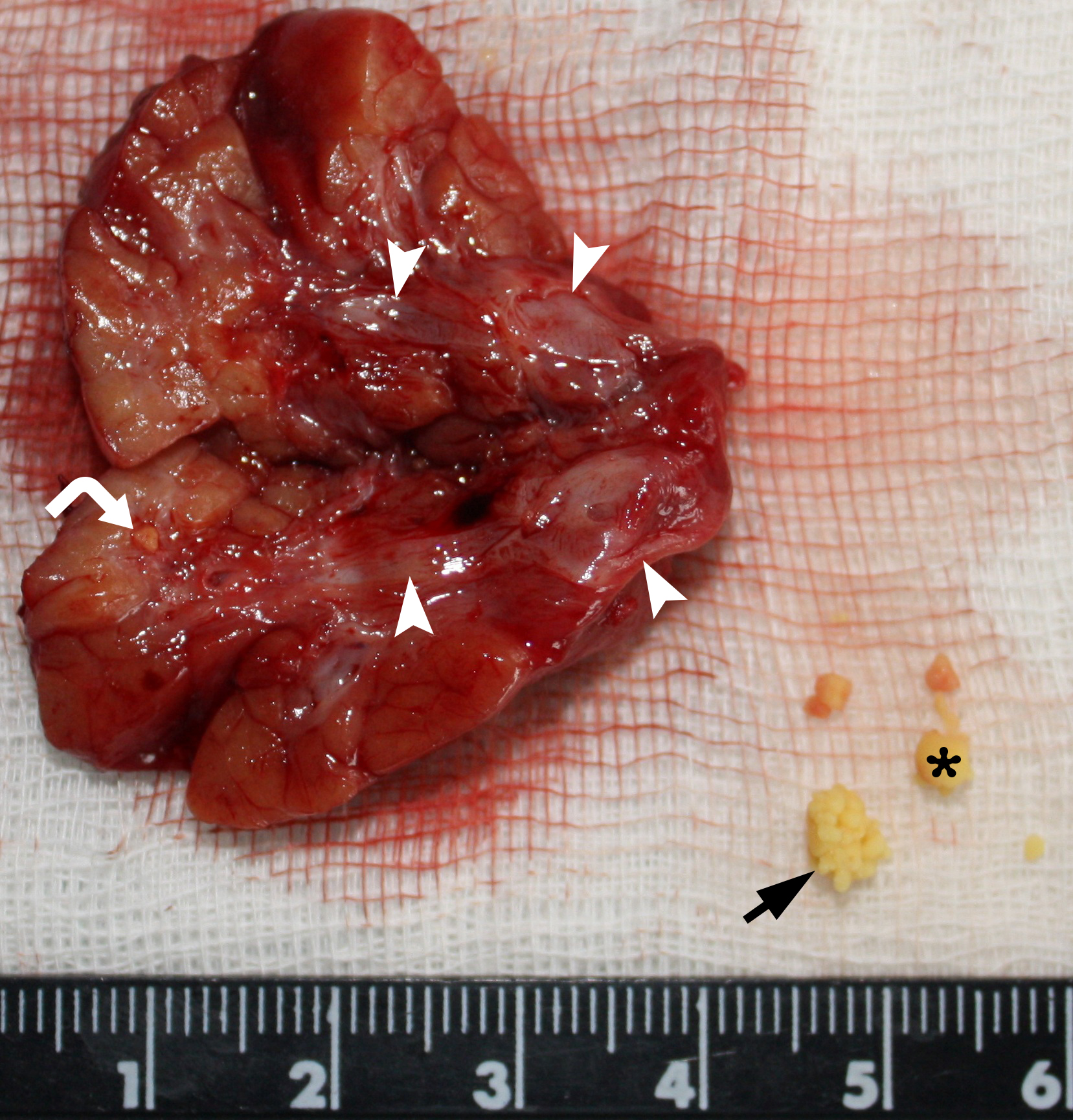
PANEL D. As the specimen and intraglandular duct were dissected longitudinally, that`s why dissected intraglandular duct (arrowheads) is visible in both parts of the gland. Also, a 1 small calculus (curved arrow) was found in the parenchymal ducts.